- See:
- See:
- Calcaneal Frx in Children
- Fatigue Fractures of the Calcaneus
- Fractures of the Anterior Process
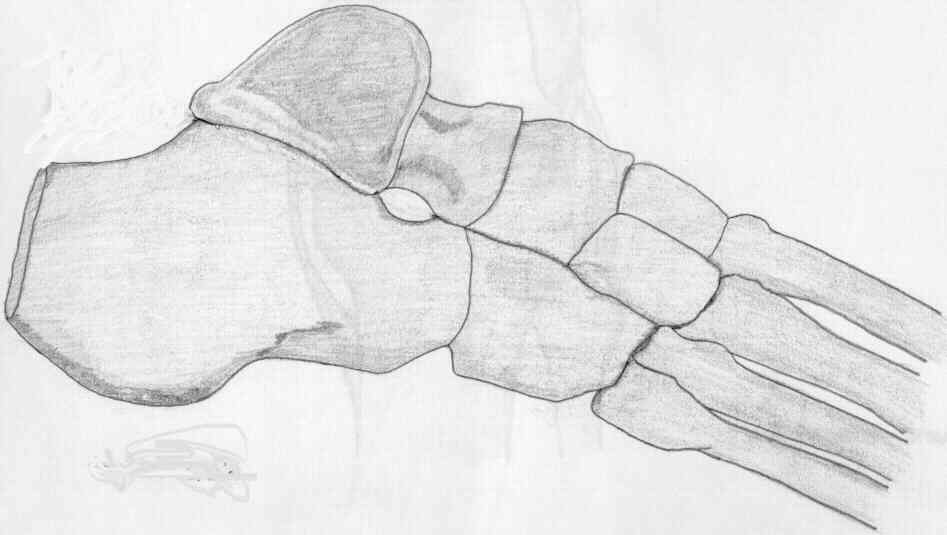
- Sub-Talar Joint
- Sustentaculuum Tali Fractures
- Discussion:
- typically results from fall from height (see mechanism)
- 2 types of frx may occur: extr-articular and intra-articular: 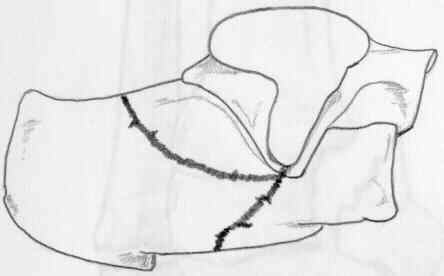

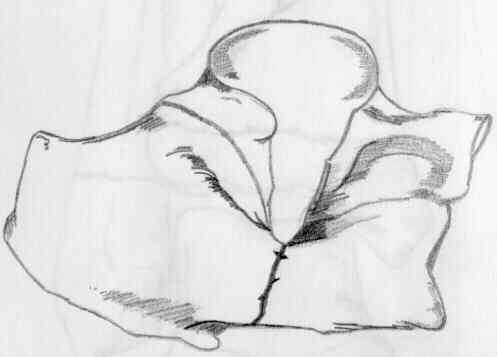
- intra-articular frx:
- secondary frx line;
- primary frx line:
- most of these involve the posterior facet (but can involve anterior and middle facets);
- sustentacular fragment (constant fragment)
- anteromedial (sustentacular) frag is rarely comminuted but varies in size;
- it remains attached to the talus by strong deltoid ligament and by the interosseous ligament lies in the interosseous sulcus
between the posterior and middle facets;
- Displacement of the Sustentacular Fragment in Intra-Articular Calcaneal Fractures
- tuberosity fragment (posterolateral fragment)
- displaces superiorly & laterally resulting in incongruity of posterior facet and widening & shortening of heel;
- further axial loading may fracture tuberosity fragment creating a supero-lateral fragment of posterior facet;
- thalamic fragment: depressed portion of the posterior facet;
- misc characteristics:
- anteriorly frx may exit laterally, usually at angle of Gissane, but it can also involve the calcaneocuboid joint;
- heel becomes shortened and widened;
- tuberosity fragment tilts into varus and is pulled proximally by the Achilles tendon;
- displaced supero-lateral fragment can impinge upon peroneal tendons;
- lateral wall becomes comminuted;
- frx extends thru posterior facet which becomes incongruous;
- talus become dorsiflexed;
- fracture classification:
- Sander's Classification:
- Rowe: types 1-5 (types 4-5 intra-articular)
- Essex Lopresti:
- extra-articular
- intra-articular
- tounge fracture
- joint depression calcaneal fracture
- associated injuries:
- frx of contra-lateral foot;
- spinal compression frx;
- soft tissue injury:
- compartment syndrome deep central compartment is involved most often in calcaneal frx;
- more common with severe comminuted fractures.
- frx blisters:
- references:
- The management of soft-tissue problems associated with calcaneal fractures.
- Compartment syndrome of the foot after intraarticular calcaneal fracture.
- Open Fractures of the Calcaneus: Soft-Tissue Injury Determines Outcome.
- Open calcaneal fractures: results of operative treatment.
- Wound healing complications in closed and open calcaneal fractures.



- Treatment Options:
- Non operative treatment:
- contraindications to open reduction:
- smoking patient who is unwilling to immediately quit smoking;
- vasculopath:
- with advanced age, diabetes, or questionable vascular exam, order non invasive vascular studies;
- most crucial measurement is degree of continuity of posterior facet, which is best determined by CT scan;
- all frx are initially treated by strict bed rest, elevation, until acute swelling has subsided;
- nondisplaced frx w/ mild or moderate decrease in Bohler's < are initially treated by early mobilization, avoidance of wt bearing for 6 weeks;
- early mobilization with protection from wt bearing is maintained until frx union occurs;
- historical treatment has included closed reduction (Bohler) w/ distraction and medial lateral compression;
- may need to be supplemented by orthotic support with a custom-molded insole, rocker-bottom shoe, or ankle-foot orthosis;
- when nonoperative treatment fails, consider sub-talar arthrodesis is often indicated;
- references:
- Intra-articular fractures of the calcaneum treated operatively or conservatively. A prospective study.
- Intraarticular calcaneal fractures. Results of closed treatment.
- Operative Versus Nonoperative Treatment of Displaced Intra-Articular Calcaneal Fractures: A Prospective, Randomized, Controlled Multicenter Trial.
- ORIF using lateral approach:
- in the review by Tufescu TV and Buckley R, the authors conducted a prospective cohort study of 169 patients who sustained intra-articular calcaneal fractures;
- they found that operatively treated fractures returned to work quicker (av 87 days sooner);
- in patients that performed heavy work:
- non op patients returned to work at 273 days vs ORIF patients who returned at av 171 days;
- ref: Age, Gender, Work Capability, and Worker's Compensation in Patients with Displaced Intraarticular Calcaneal Fractures.
- Primary Subtalar Fusion for Calcaneal Fracture
- Percutaneous Fixation:
- may be indicated for patients with inadequate soft tissues (diabetics with frx blisters) where risk of dehissence is high;
- main goal is to regain calcaneal height and width and to take the calcaneus out of varus alignment;
- no attempt is made to reconstruction the articular surface;
- technique:
- manual position across the calcaneal body;
- large threaded Steinman pin is placed through the posterior superior portion of the calcaneal tuberosity;
- distraction helps restore calcaneal width and height
- longitudinal traction is applied across the Steinman pin w/ a valgus vector applied as well;
- threaded Steinman pin is inserted through the posterior inferior corner of the calcaneus, across posterior facet and into the talar body;
- this stabilizes the valgus reduction;
- threaded Steinman pin is inserted through the posterior calcaneus into the cuboid;
- technique:
- prone position;
- distraction screws: ex fix across the calcaneal tuberosity, distal tibia, and/or cuboid and the talus;
- transcalcaneal rod (from below) which pushes and elevated fracture fragments;
- this pushes up depressed parts of subtalar joint;
- may also use lateral pin to manipulate the fracture fragments;
- cannulated screw: inserted from latearal to medial into the sustentaculum tali;
- Bruce Ziran/P. Bosch: of 25 frxs, 12 patients reported little or no pain, 7 patients had moderate pain, and 2 patients had severe pain;
- references:
- Closed reduction and percutaneous pinning for comminuted intra-articular fractures of the calcaneus: Preliminary results.
Bruce Ziran and P. Bosch. 15th Annual Meeting of the Orthopaedic Trauma Association, 1999.
- Treatment of Displaced Intra-Articular Calcaneal Fractures with Closed Reduction and Percutaneous Screw Fixation
- Complications of Treatment
Current Concepts Review. Intra-Articular Fractures of the Calcaneus.
The medical approach for calcaneal fractures.
Intra-articular fractures of the calcaneus. A critical analysis of results and prognostic factors.
Intra-articular fractures of the calcaneum. Part I: Pathological anatomy and classification.
Mechanism and pathoanatomy of the intraarticular calcaneal fracture.
Fractures of the calcaneum: the anterolateral fragment.
Computed tomographic assessment of soft tissue abnormalities following calcaneal fractures.
Magnetic resonance imaging evaluation of calcaneal fat pads in patients with os calcis fractures.
Intra-articular fractures of the calcaneus: Present state of the art.
Intra-articular fractures of the calcaneus.
Fractures of the calcaneus: open reduction and internal fixation from the medial side a 21-year prospective study.
Operative Compared with Nonoperative Treatment of Displaced Intra-Articular Calcaneal Fractures. A Prospective, Randomized, Controlled Multicenter Trial
Open Fractures of the Calcaneus: Soft-Tissue Injury Determines Outcome.
Long-Term Functional Outcomes After Operative Treatment for Intra-Articular Fractures of the Calcaneus
The association between subtalar joint motion and outcome satisfaction in patients with displaced intraarticular calcaneal fractures.