
- See:
- Grice Arthrodesis
- Primary Subtalar Fusion for Calcaneal Fracture
- Sub-Talar Joint
- Triple Arthrodesis
- Discussion:
- in the series by Mann, et al (1998), 48 subtalar fusions were performed w/ 93% satisfactory results;
- the authors noted that transverse tarsal motion was decreased by 40%, dorsiflexion was reduced by 30%;
- mild degenerative changes were seen in about 1/3 patients at either the ankle or transverse tarsal joints;
- subtalar degenerative disease:
- subtalar arthrodesis results in less rigid foot (does not tie up remainder of peri-talar articulations);
- subtalar arthrodesis limits talonavicular motion to about 26%, and limits calcaneocuboid motion to about 56%;
- talonavicular fusion will limit subtalar motion to about 9%;
- calcaneocuboid fusion decreases talonavicular motion down to 67% and subtalar motion down to 92%;
- soft tissue procedures:
- FDL tendon transfer to navicular or first cuneiform has been advocated to improve function and stabilize talonavicular joint;
- ref: Subtalar arthrodesis with flexor digitorum longus transfer and spring ligament repair for treatment of posterior tibial tendon insufficiency.
- contraindications:
- w/ significant forefoot varus, a subtalar arthrodesis is not sufficient (requires triple arthrodesis);
- Isolated subtalar arthrodesis
- PreOp Planning and Radiographs:
- optimal position of subtalar fusion
- surgical instruments:
- currettes, lamina spreader w/ and w/o teeth, osteotomes, peri-osteal elevators, spade retractors, homan retractors, and curved creigo elevators;
- Positioning:
- supine, w/ bumb under hip;
- prep for bone graft;
- Surgical Incision:



- mark out base of 5th metatarsal and tip of lateral malleolus;
- select point halfway between the two and make an oblique incision which parallels subtalar joint line over sinus tarsi; (see Ollier Incision);
- alternatively make the incision from the tip of the fibula to the base of the 4th metatarsal;
- avoid the sural nerve which lies 1-2 cm beneath the distal tip of the fibula;
- avoid cutting toe extensors which lie anterior and peroneal tendons which lie posterior;
- open the peroneal tendon sheath and expose the brevis tendon;
- partially open the extensor tendon sheath;
- distally based EDB flap:
- EDB is freed from its insertion & reflected distally, w/ care to preserve the nerve supply;
- outline of EDB is completed allowing creation of a distally based EDB flap;
- in medial & dorsal aspects of EDB, keep dissection subperiosteal to avoid neurovascular damage;
- NV bundle enters approx 1.5 cm medial & distal to anterior process of the calcaneus;
- retract peroneal tendons out of their tendon sheath plantarly & laterally;
- continue dissection to cuboid and distal calcaneus thru deep portion of peroneus sheath;
- EDB belly is delivered out of Sinus Tarsi by sub-perosteal dissection;
- remove the fibro-fatty contents of the sinus taris w/ a rounguer;
- identify the calcaneocuboid joint which is found just distal to the anterior beak of the calcaneous - avoid entering into the joint;
- the talo-navicular joint lies superior and medial to calcaneocuboid joint;
- identify neck of the talus, and elevate the extensor tendons off the neck;
- insert a spade over the neck / under the extensor tendons which helps retract the N/V bundle;
- Disruption of Joint Surfaces:
- insert a Creigo curved elevator deep to the peroneal tendon and around calcaneus at the level of the sub talar joint;
- consider removing the lateral talar process to better expose the posterior facet;
- joint capsule of talocalcaneal joint is incised & laminar spreader is inserted into sinus tarsi to expose entire subtalar articulation;
- excise articular cartilage & subchondral bone of subtalar joint:
- care should be taken to insure excision of articular catilage from anterior, middle, and posterior facet;
- all of the non articular surfaces are decorticated;
- avoid excessive bone resection since this will decrease the subtalar joint height and will disrupt the articular relationship of the talo-naviulcar joint;
- if there is a fixed valgus or varus deformity additional bone is removed from either the medial or lateral sides of the joint;
- Insertion of Bone Graft: 
- references:
- Treatment of Severe, Painful Pes Planovalgus Deformity with Hindfoot Arthrodesis and Wedge-Shaped Tricortical Allograft
- Triple arthrodesis: is bone grafting necessary? The results in 100 consecutive cases.
- Subtalar distraction bone block fusion for late complications of os calcis fractures.
- Subtalar distraction arthrodesis using interpositional frozen structural allograft.
- Hindfoot arthrodesis in adults utilizing a dowel graft technique.
- Isolated talocalcaneal arthrodesis. A technique using moldable bone graft
- Subtalar distraction arthrodesis using interpositional frozen structural allograft.
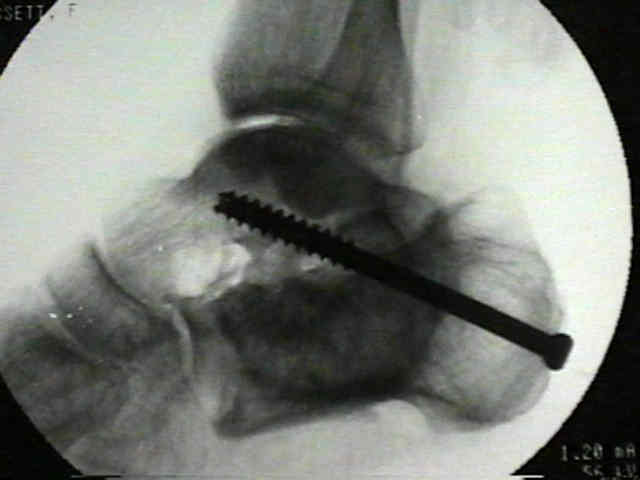
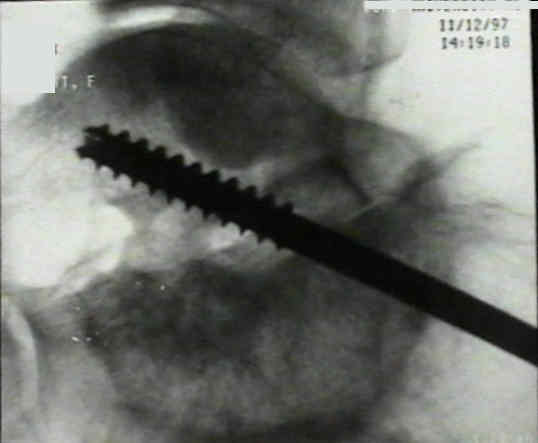
- Position the Ankle and Insert Hardware;
- see: optimal position of fusion::
- hold ankle in neutral dorsiflexion/plantar flexion & calcaneus in sl valgus;
- do not change this position;
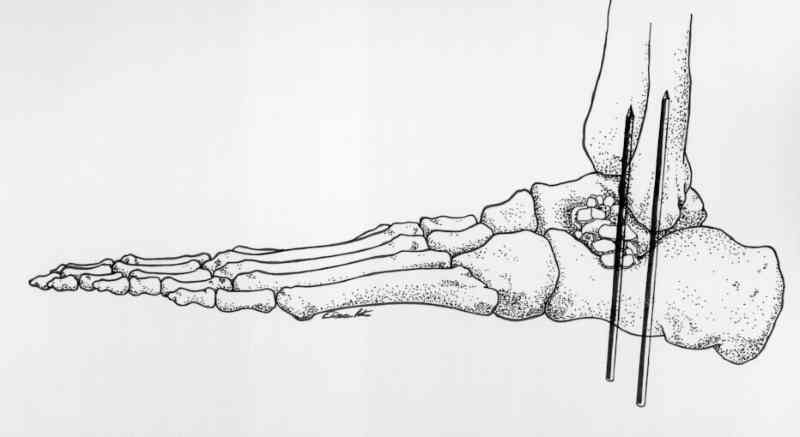
- anterior to posterior screw insertion:
- insert pin medial to anterior tibial tendon from talar neck into calcaneus;
- the surgeon's finger is passed into the lateral incision and palpats the drill/trocar complex to ensure that the drill is centered over the talar neck;
- if fixation screw is inserted w/ ankle in plantar flexion and is located too close to anterior margin of tibia, it may block dorsiflexion;
- visualized pin as it goes thru sinus tarsi region into calcaneus;
- bulge of the pin under the skin of the heel region is then felt and the pin is retracted back about 2 cm;
- advantages:
- allows insertion of long threaded lags screws;
- disadvantages:
- is associated w/ AVN of the talar head;
- may cause ankle impingement in dorsiflexion;
- posterior to anterior screw insertion:
- often requires use of short threaded lag screws;
- does not seem to cause heel pad symptoms if the incision and screw are kept just above the heel pad;
- consider placing a "tibial tunnel ACL guide" thru the lateral incision and onto the center of the posterior facet so that the guide
pin can be reliably placed across the subtalar joint;
- prior to guide pin placement, place the subtalar joint in 5 deg of valgus;
- in many cases, a washer is required inorder to achieve good screw fixation;
- reference:
- Placement of screws in subtalar arthrodesis: a simplified technique.

- Post Operative Management:
- patients are kept NWB on crutches for 6 weeks;
- pt is then allowed to bear wt in cast as tolerated for second 6 week period;
- at 12 weeks the cast is removed;
- Complications:
- improper positioning of subtalar joint;
- w/ excessive hindfoot valgus, pt may complain of pain in arch region;
- hindfoot varus can lead to significant lateral margin foot pain;
- fixation screw may block ankle dorsiflexion
Subtalar fusion for isolated subtalar disorders. Preliminary report.
Selective tarsal arthrodesis: In vitro analysis of the effect on foot motion.
The transverse tarsal joint and its control.
Tibiotalocalcaneal arthrodesis for arthritis and deformity of the hind part of the foot.
Subtalar stabilization of the planovalgus foot by staple arthroereisis in young children who have neuromuscular problems.
Isolated subtalar arthrodesis.
A comprehensive review of subtalar arthrodesis.
Original Text by Clifford R. Wheeless, III, MD.
Last updated by Clifford R. Wheeless, III, MD on Sunday, April 12, 2015 3:34 pm