
- see anatomy of the scapula

- most common scapular frx are frx of the body, followed by the neck, glenoid, and acromion;
- associated injuries: seen in upto 80-90% of patients;
- pulmonary injuries and pneumothorax (23%) and pulmonary contussion;
- clavicle frx (23%), which represents a floating shoulder injury;
- shoulder dislocation either anterior or posterior
- brachial plexus injuries and axillary artery injury;
- axillary artery injury:
- rib fractures
- references:
- Multiple trauma and scapula fractures: so what?

- Triple and Quadruple Disruptions of the Superior Shoulder Suspensory Complex
- Scapular Neck Frx:
- make up about 2/3 of scapular fractures;
- usually these frx are impacted and extra-articular,
and have good prognosis for healing;
- classification:
- type I - nonangulated, nondisplaced
- type IIa - shortened / displaced > 1 cm
- type IIb - Angulated > 40 deg
- surgical indications:
- greater than 1 cm medial displacement;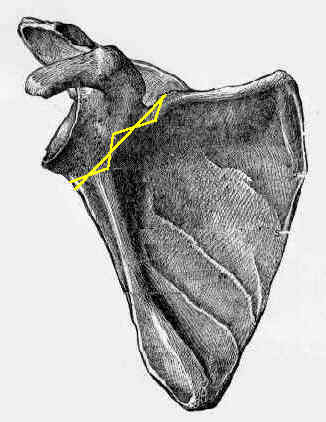
- greater than 40 deg angulation;
- nondisplaced - nonoperative treatment yields good results, no function limitation;
- displaced - nonoperative treatment yields significant functional disability;
- associated injuries:
- rib fractures
- hemo/pneumothorax
- flail chest/tension pnemaothorax
- brachial plexus injuries
- vascular injuries
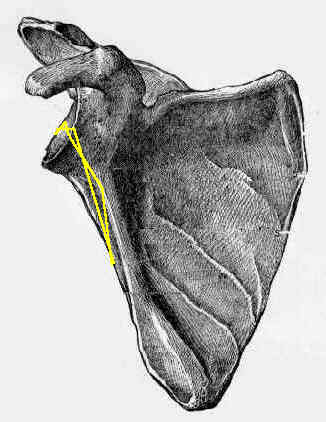
- Glenoid Lip Frx:
- usually involve either the anterior or posterior lip of the glenoid and are oriented vertically (and exit inferiorly);
- large lip frxs of glenoid are usually assoc w/ subluxation or partial dislocation of the head of the humerus;
- Glenoid Fossa Frx: 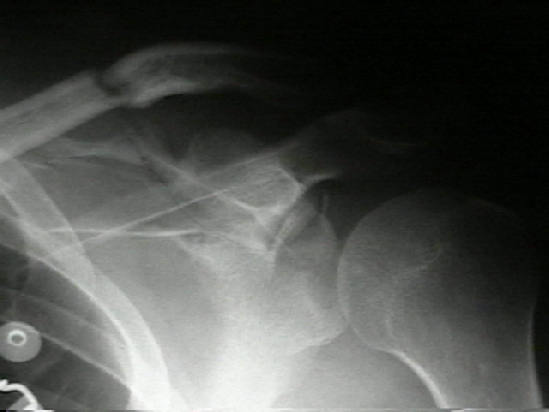
- uncommon frx comprising about 10% of scapular fractures;
- glenoid fractures typically present w/ transverse frx thru the glenoid;
- some frxs will extend medially across scapula and exit just medial to the coracoid or will
exit at the medial aspect of the scapula;
- Ideberg Classification
- Type I- Anterior avulsion fractures
- Type II- Tranverse, inferior glenoid
- Type III- Tranverse, superior glenoid
- ref: Arthroscopic-assisted reduction and percutaneous cannulated screw fixation for Ideberg type III glenoid fractures: a minimum 2-year follow-up of 18 cases.
- Type IV- Transverse, through body
- Type V- Combo of types II and IV
- common fracture patterns:



- Radiology:
- AP of Shoulder:
- it is essential to rule out articular involvement with a high quality AP view in which there is no overlap of the humerus over the glenoid;
- ideally, the view should be purely tangential to the glenoid;
- 45 deg cephalic tilt allows evaluation of coracoid fractures;
- Apical Oblique View:
- CXR: rib fractures
- Systematic Review:
- need to carefully assess the entire scapular body and spine, the acromion, coracoid, and finally the glenoid;
- need to asses each articulation: glenohumeral, AC joint, and scapulo-thoracic;
- degree of medialization, extent of comminution, and angular relationship of the glenoid to the body;
- CT Scanning:
- allows more accurate assesment of articular step off, as well as displacement and angulation of glenoid neck;
- CT scanning is particulary helpful in evaluation of intra articular glenoid frx;
- Non Surgical Treatment:
- vast majority of scapula fractures may be treated non operatively,
- closed reduction of these frx is usually not possible;
- treatment consists of support of a sling and early motion;
- most fractures will heal by 6 weeks;
- if an "operative scapular frx" is treated non operatively, the patient may develop abductor weakness and subacromial impingement;
- outcomes:
- in the report by Romero J, et al, the authors analyzed the effect of associated shoulder girdle injury on glenoid displacement and
the influence of glenoid malalignment on clinical outcome;
- 19 patients with scapular neck fractures were reviewed clinically and radiologically at a mean of 8 years after injury;
- none of them has developed nonunion of the scapular neck, and only one showed radiological signs of mild degenerative joint disease.
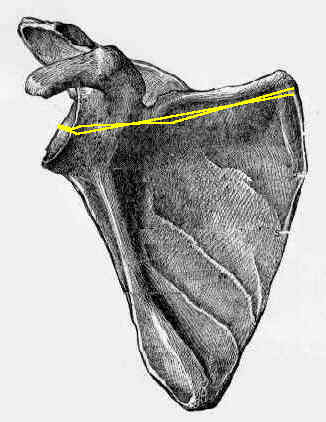
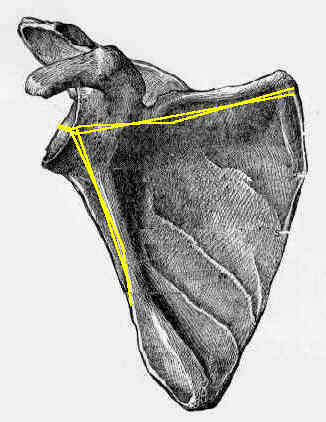
- glenopolar angle (GPA), which assesses the rotational malalignment of the glenoid about an anteroposterior axis perpendicular
to the scapular plane on plain X-rays was measured less than 20° in six patients;
- 3 of them had sustained an associated clavicular fracture or AC joint dislocation;
- other 3 patients had permanent severe malalignment of the glenoid neck in the absence of an associated shoulder girdle injury.
- 5 patients with GPA less than 20° complained of moderate or severe pain, whereas of the 13 patients with mild or no glenoid rotational
displacement or medial displacement alone, 11 patients had no or mild pain, and only 2 had moderate or severe pain (p = 0.0095);
- 5 patients presented with reduced activities of daily living, 4 of them had severe glenoid rotational displacement;
- loss of motion was found in only 2 patients, and both had a severely displaced glenoid neck (p = 0.088).
- references:
- Scapular neck fracture - the influence of permanent malalignment of the glenoid neck on clinical outcome
- Outcomes of Nonoperatively Treated Displaced Scapular Body Fractures
- Surgical Treatment of Glenoid Frx:
- indications:
- need to distinguish glenoid rim frx from glenoid fossa frx;
- glenoid rim frx which are displaced more than 10 mm or those which are displaced and involve more than 25% of joint surface
are likely to be associated w/ instability and require fixation;
- intra articular glenoid frx w/ subluxation & instability of humeral head is a definite indication;
- glenoid fossa fractures which are displaced more than 5 mm require fixaiton;
- Implants:
- 3.5mm cortex screws or 4.0mm cancellous screws as lag screws
- 1/3 tubular plate may be applied below glenoid to lateral border of scapula as a butress;
- Surgical Approach:
- anterior rim frxs are approached anteriorly and posterior rim frx are approach posteriorly;
- transverse glenoid fractures may be directly reduced through the anterior approach and have fixation via percutaneously inserted
screws from above (thru the deltoid);
- Anterior Approach in Fractures of the Glenoid;
- for fractures of the anterior and inferior margins of the glenoid, the deltopectoral approach may be chosen;
- reduction of inferior glenoid fractures can be difficult due to proximity of axillary nerve;
- osteotomy of the coracoid may be necessary for improved exposure;
- reattach coracoid with 4.5 mm cortex screw and absorbable washer to avoid splitting of the coracoid tip;
- Surgical Treatment of Extra-articular Scapular Frx:
- Inidcations:
- depressed acromion fractures that encroach on the subacromial space and interfere with rotator cuff function;
- scapular neck frx w/ severe angluation (more than 40 deg) or w/ more than 1 cm of medial translation;
- extra-articular frxs of scapular neck, along w/ frx of acromion or w/ frx of coracoid (esp if AC separation is present);
- if the AC ligaments are torn, and the CC ligaments are attached to the frx fragment then an AC disruption will result;
- extra-articular frxs of scapular neck w/ associatted w/ frx of clavicle;
- w/ concomitant fractures of the scapular neck & clavicle, the clavicle is approached first & fixed with a IM clavicular pin;
- this should partially reduce the scapular neck frx & possibly allowing the scapular neck frx to be treated non operatively;
- Treatment Considerations:
- w/ glenoid neck frxs, (articular surface in intact) frx extends from suprascpular notch area across neck to lateral border of scapula;
- glenoid neck frx is often displaced but an intact clavicle & AC joint will limit displacement and provide stability;
- implant of choice is often a contoured 3.5 pelvic reconstruction plate which is applied to the posterior border of the glenoid
and the lateral border of the scapula;
- Implant:
- 1/3 tubular plate, 3.5 mm DCP, or LC-DCP for fixation of Clavicle;
- 3.5 mm DCP or LC-DCP;
- contoured 3.5 pelvic reconstruction plate;
- 4.0 mm cancellous bone screws as lag screws;
- Posterior Approach to Shoulder
- prone or lateral position with the arm supported;
- for frx of posterior aspect of glenoid & lateral scapular margin
- curved skin incision starts at lateral prominence of acromion, courses medially along scapular spine & caudally to inferior angle of Scapula;
- detach of deltoid from scapular spine and retract laterally;
- deepen approach thru interval between infraspinatus & teres minor;
- original Judet posterior approach involved elevation of belly of infraspinatus which was then reflected laterally to expose whole infraspinatus fossa;
- reduction can be achieved using pointed reduction forceps;
- ref: Modified Judet approach and minifragment fixation of scapular body and glenoid neck fractures.
Radiographic and geometric anatomy of the scapula.
Fracture of the body, neck, or spine of the scapula. A long-term follow-up study.
The fractured scapula: importance and management based on a series of 62 patients.
Fractures of the scapula. An analysis of forty cases and a review of the literature.
Pneumothorax complicating fracture of the scapula.
Scapular fractures. Analysis of 113 cases.
Fractures of the scapula: a review of 53 fractures.
The operative treatment of scapular fractures.
Scapular fractures and dislocations: diagnosis and treatment.
A Modified Judet Approach to the Scapula.
Fractures of the scapula: a retrospective study of 40 fractured scapulae.
Fractures of the acromion and the lateral scapular spine.