
- See:
- Associated Transverse and Posterior Wall Frx
- Classification and Column Theory
- Discussion:
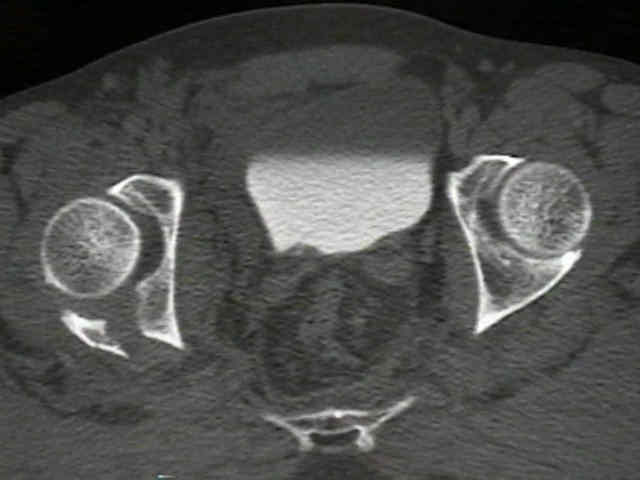
- most common type of acetabular frx (up to 50% of acetabular fractures will contain a posterior
wall fragment);
- posterior wall frxs involve the posterior articular surfaces, often w/ retroacetabular surface and
sometimes entire surface;
- frx of posterior rim & posterior column may be seen in MVA from posteriorly directed dashboard impact;
- hips w/ > 40-50% involvement of posterior wall (as per CT scan) or w/ posterior subluxation are unstable and
require ORIF to restore acetabular wall;
- posterior wall and posterior dislocation of hip;
- reduction needs to be within 6 hours of injury;
- CT only need be performed following closed hip reduction;
- work up of acetabular frx and associated injuries:
- inspection of soft tissues:
- GYN / urinary / rectal injuries: RUG vs. suprapubic catheter placement;
- neurologic injury:
- w/ this injury, the sciatic nerve may be injured about 30% of patients;
- be sure to document even subtle signs of injury;
- ref: Somatosensory evoked potential monitoring in the surgical treatment of acute, displaced acetabular fractures. Results of a prospective study.
- transverse frx (most common);
- posterior dislocation of hip;
- posterior dislocation with femoral head fracture:
- if femoral head fragment is above the fovea, then attached ligamentum teres prevents reduction of the
femoral head fracture;
- with small infrafoveal fragments, a posterior approach may allow fixation or debridement of the femoral head fragment;
- anteroposterior compression fractures;
- PCL rupture (may occur along w/ posterior wall frx when dashboard injury is the mechanism of injury);
- Radiographic Studies:
- internal (obturator) oblique view:
- visualizes iliopubic (anterior) column of pelvis & posterior rim;
- demostrates the fracture fragment, acetabular defects and degree of displacement;
- note whether there are intra-articular frx fragments;
- note degree of comminution:
- most posterior wall fractures will have some degree of posterior comminution;
- w/ isolated posterior wall frx, ilioischial line remains intact;
- note that comminution of the posterior wall fragment is a poor predictor of outcome (3 or more fragments
indicates poor prognosis);
- posterior wall fracture extending into the acetabular roof also indicates negative prognosis;
 ***
*** 


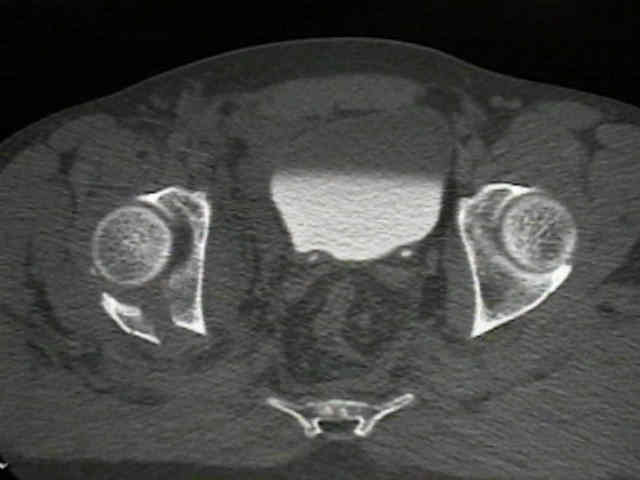
- CT Scan:
- hips w/ less than 34% of the remaining posterior wall are generally unstable;
- hips w/ more than 55% of the remaining posteiror wall are generally stable;
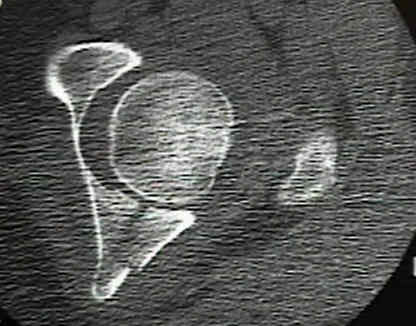
- note degree of comminution;
- single posterior fragment is present in 30%;
- multiple fragment fractures occur in about 30%;
- osteochondral depression fractures of the posterior wall;
- references:
- Computed tomography evaluation of stability in posterior fracture dislocation of the hip.
- Stability of posterior fracture-dislocations of hip. Quantitative assessment using computed tomography.
 **
** 
- Non Operative Treatment:
- indications:
- stable fractures (less than 30-50%) which are demonstrated to be stable under flouroscopic evaluation;
- congruent reduction w/ assurance that incarcerated fracture fragments are not present (as determined from fine cut CT scan);
- references:
- Computed tomography as a predictor of hip stability status in posterior wall fractures of the acetabulum.
- Outcomes of posterior wall fractures of the acetabulum treated nonoperatively after diagnostic screening with dynamic stress examination under anesthesia.
- Can experts in acetabular fracture care determine hip stability after posterior wall fractures using plain radiographs and computed tomography?
- Nonoperative Treatment of Posterior Wall Acetabular Fractures After Dynamic Stress Examination Under Anesthesia: Revisited.
- Examination Under Anesthesia for Evaluation of Hip Stability in Posterior Wall Acetabulum Fractures..
- Surgical Considerations:
- indications for ORIF:
- irreducible fracture dislocation;
- incarcerated osteochondral fragments:
- in some cases, small fragments which lie in the lower half of the acetabulum do not require removal;
- ref: Intra-articular Fragments in Acetabular Fracture-Dislocation
- hip instability;
- defect in the posterior wall of more than 50% (associated w/ instability even if instability is not apparent on
static radiographs);
- defects of between 30-50% may or may not be stable;
- often the status of the posterior capsule determines whether the hip is stable;
- elderly patients:
- fractures in elderly patients and those with extensive comminution are more likely to have a poor clinical result;
- ref: Results of Operative Treatment of Fractures of the Posterior Wall of the Acetabulum
- other considerations:
- references;
- Outcomes of posterior wall fractures of the acetabulum treated nonoperatively after diagnostic screening with dynamic stress examination under anesthesia.
- Does Early Fixation of Posterior Wall Acetabular Fractures Lead to Increased Blood Loss?
- Surgical Technique:
- prone positioning:
- posterior wall fractures that extend from the greater and or lesser sciatic notch are usually best operated on w/ prone
positioning;
- w/ posterior instability, prone position ensures hip reduction;
- prone position keeps the hip in extension which reduces sciatic nerve tension;
- be sure that the patient is placed on a flouro table and be sure to run through all of the important flouroscopic views prior to
prepping the patient;
- implants and tools for posterior wall fracture:
- 3.5 mm cortical screws, 4.0 mm cancellous bone screws, 3.5 mm reconstructed plate, curved,
- spiked ball pusher, T handle chuck and schanz half pin, flouro OR table;
- synthes spring plates
- bone grafting: indicated for comminuted posterior wall fractures;
- Surgical Exposure:
- Kocher Langenback incision:
- a sliding trochanteric osteotomy may be required if there is cranial extension of the wall fragment;
- releasing 1 cm of the gluteus insertion onto the femur widens the posterior exposure;
- knee should be flexed to protect the sciatic nerve;
- dislocation of femoral head:
- Surgical Hip Dislocation for Exposure of the Posterior Column
- Patients undergoing surgical hip dislocation for the treatment of acetabular fractures show favourable long-term outcome.
- deep exposure:
- schanz screw (w/ T chuck handle) can be inserted into the greater trochanter, inorder to distract the femoral head for
improved exposure;
- joint is debrided & irrigated to remove all loose fragments;
- articular surfaces are inspected & impactions of articular surface are elevated;
- in some cases, the posterior wall fragment may be displaced anteriorly and held tethered by the anterior capsule
(ligament of Bigelow);
- small fragments may be discarded, but save & reduce all fragments since significant posterior wall defects may lead
to hip instability;
- capsular attachment to the posterior wall fragment should be preserved to maintain circulation;
- superior fracture extension of the posterior wall:
- consider trochanteric slide osteotomy in order to
- avoid stretch on the superior gluteal neurovascular bundle;
- avoid direct damage to the medius and minimus muscles;
- references:
- Modified Kocher-Langenbeck approach for the stabilization of posterior wall fractures of the acetabulum.
- Modified "2-portal" kocher-langenbeck approach: a minimally-invasive procedure protecting the short external rotator
- Management of acetabular fractures with modified posterior approach to spare external hip rotators.
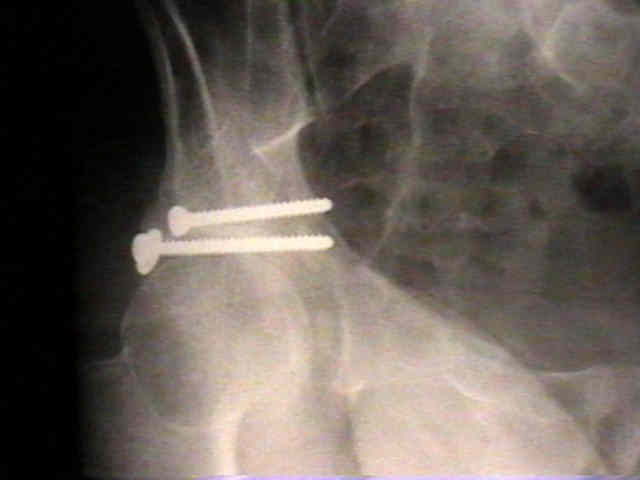
- fixation w/ lag screws:
- fixation w/ lag screws is inferior to fixation w/ lag screws and a contoured plate;
- best indication for lag screw fixation is large non comminuted posterior wall fragment;
- two synthes 3.5 mm cortical screws are inserted after the outer cortex has been over-drilled w/ a 3.5 mm drill bit;
- it is important to aim the drill bit perpendicular to the fracture site (rather than perpendicular to the cortex site);


- hazards:
- danger zone of the acetabulum (screw penetration of joint):
- consider role of hip arthroscopy;
- note: its easy for screws inserted into retroacetabular space to enter joint;
- screws are normally directed away from the joint, oblique to the retroacetabular surface;
- retrograde drilling of frx frag may avoid joint penetration, however, requires stripping fragment from hip capsule,
(removing its blood supply);
- radiographic methods to determine articular penetration:
- multiple flourscopic views including cross table lateral view and the Judet iliac view are often the most useful views;
- flouroscopy w/ intra-articular contrast dye and moving the hip w/o crepitus are other methods to avoid joint
penetration;
- using flouroscopy to achieve "end on" view of lag screws;
- reference:
- Radiographic diagnosis of screw penetration of the hip joint in acetabular fracture reconstruction.
- Danger Zone of the Acetabulum.
- fixation w/ reconstruction plate (and lag screws or sping plate):
- most indicated for comminuted posterior wall frx;
- butress plate (8 hole 3.5 mm recon plate) is placed along posterior rim of acetabulum (placed from superior pole of ischium
to inferior iliac wing);
- plate is curved so that it roughly parallels rim of acetabulum (it should be precontoured on a model preoperatively);
- undercontouring of the plate helps butress the fragment;
- generally two screws are placed above and below acetabulum;
- generally two lag screws are inserted midway between the reconstruction plate and the edge of the posterior wall;
- note: its easy for screws inserted into retroacetabular space to enter joint;
- see: danger zone of the acetabulum:
- screws are normally directed away from the joint, oblique to the retroacetabular surface;
- referencs:
- Fixation of marginal posterior acetabular wall fractures using locking reconstruction plates and monocortical screws.
- The Use of Cervical Vertebrae Plates for Cortical Substitution in Posterior Wall Acetabular Fractures
- Fractures of the posterior wall of the acetabulum: treatment using internal fixation of two parallel reconstruction plates.



- spring plate: (synthes spring plates)
- indicated for comminution;
- use a four hole one third tubular plate;
- one end of the plate holes is cut out and bent 90 deg;
- the plates are contoured to fit the bone;
- the two prongs are inserted into the acetabulum 5 mm from its edge;
- the plates are secured to the pelvis at the most posterior hole;
- following application of the plate, the 3.5 recon plate is placed over the spring plate;
- there is some controversy as to whether spring plates offer any significant stability;
- spring plates create a special risk of intra-articular compromise of the joint surface;
- if the "hooks" of the plate are too long or malpositioned, the femoral head may be at risk for damage;
- ref:
- The Use of a T-Plate as "Spring Plates" for Small Comminuted Posterior Wall Fragments.
- Use of Spring Plates in Fixation of Comminuted Posterior Wall Acetabular Fractures
- Supplemental Superior Buttress Plating for the Treatment of Posterosuperior Wall Acetabulum Fractures
- bone grafting:
- bone grafting is often required to support impacted articular fragments;
- articular impaction is managed with elevation and application cancellous bone graft;
- large free fragments are reattached and small fragments removed;
- avoid fracture gaps;
- Post Op:
- postoperative CT scan allows optimal evaluation of surgical reconstruction;
- need to limit postoperative hip flexion inorder to limit stress on the posterior wall fragment;
- references: Computed tomographic assessment of fractures of the posterior wall of the acetabulum after operative treatment
- Complications:
- this fracture type is associated w/ a high complication rate;
- iatrogenic sciatic nerve injury may occur and may be prevented by constant knee flexion during the case and by intraoperative
SSEP monitoring;
- loss of fracture fixation is a common complication;
- after ORIF of posterior wall frx, post traumatic osteoarthitis may occur in up to 20% of patients
- non union:
- ref: Indomethacin prophylaxis for heterotopic ossification after acetabular fracture surgery increases the risk for nonunion of the posterior wall.
Percutaneous retrograde posterior column acetabular fixation: is the sciatic nerve safe? A cadaveric study.
Biomechanical consequences of fracture and repair of the posterior wall of the acetabulum.
Comminuted Fractures of the Posterior Wall of the Acetabulum. A biomechanical evaluation of fixation methods.
Posterior Acetabular Wall Fractures: a technique for screw placement.
Hip Arthroscopy to Remove Loose Bodies After Traumatic Dislocation.
Determinants of functional outcome after simple and complex acetabular fractures involving the posterior wall.
Surgical techniques-How do I do it? Open reduction and internal fixation of posterior wall fractures of the acetabulum