
Discussion
- note that some of the problems seen in dysplasia are frequently encountered in revision THR;
- indications for acetabular revision:
- sepsis, component malposition, impingement, polyethylene wear, pelvic osteolysis, recurrent dislocation, progressive protrusio, and component loosening;
- evaluation of the painful THR
examination:
- examination for loosening
- previoius incisions;
- contracture of the flexors and adductors (adds to complexity of the case);
- leg-length inequality is noted;
- neurovascular status of the limbs is recorded (EMG can be ordered if necessary);

- power of the abductor muscles is noted;
- marked Trendelenburg gait may indicate that abductors are non functional;
preop planning » (radiographs, equipment, implant selection);
- radiographic evaluation of acetabular components: (Paprosky Classification)
- classification of defects
- extraction instruments
- cell saver;
- rule out infection:
- in addition to preoperative hip aspiration, consider culture of nares since preoperative staph aureus nasal carriage is associated with postoperative infection;
- intraoperative cultures and cell count:
- WBC count of less than 3000/?L indicates the absence of infection
- WBC count of greater than 10,000/?L indicates the presence of an infection;
- WBC cout of between 3000 and 10,000, base decision on the C-reactive protein level frozen section;
- references:
Surgical Considerations
acetabular exposure »
- w/ hybrid THR, typically the femoral stem is first removed (to improve exposure) but the cement is left in place (to reduce blood loss);
- if exposure is not optimal, then consider trochanteric osteotomy;
- entire circumference of the acetabular component must be visualized;
- polyethylene is then removed (may be performed w/ corkscrew or with insertion of 6.5 mm screw thru the polyethylene and against the metal cup);
- if screws are present, these are removed;
- ref: A technique of revision of failed acetabular components leaving the femoral component in situ.
management of osteolysis »
- note that in cases of acetabular osteolysis, the metal cup will often will have fixed ingrowth into the acetabulum;
- attempts to revise the component in these cases, may end up removing significant amounts of bone or may even risk fracture;
- references:
technique for cup removal »
- surgeon needs to have a "back up plan" if component removal results in acetabular fracture;
- references:
protrusio »
- w/ mild protrusio, routine methods can be used to remove the acetabular component, but with severe protrusio consider an intrapelvic approach (to avoid vasular, nerve, and or bowel injury);
- reference:
bone grafting of acetabular defects »
- management of pelvic discontinuity
- reference:
Acetabular Component Insertion and Grafting Options
general considerations:
- need to determine the level of the true acetabulum;
- homan retractor is placed in the obturator foramen as a reference for the inferior aspect of the acetabulum;
- sequential reaming is carried out until the anterior and posterior columns are engaged by the reamer;
- non biologic fixation:
- antiprotrusio cage: (w/ or w/o structural allograft);
- impaction grafting with or without an antiprotrusio cage;
- cemented polyethylene cup
- superior structural allograft w/ cemented polyethylene cup;
- total acetabular allograft;
- cementing a liner into a well fixed cup:
- need to make sure that the polyethylene cup is smaller than the shell;
- there needs to be at least some minimal roughness to allow for adequate cement fixation;
- references:
- A constrained liner cemented into a secure cementless acetabular shell.
- A biomechanical analysis of polyethylene liner cementation into a fixed metal acetabular shell.
- Cementation of a Polyethylene Liner into a Metal Acetabular Shell: A Biomechanical Study
- Dislocation after polyethylene liner exchange in total hip arthroplasty.
- Cementation of a polyethylene liner into a metal shell: Factors related to mechanical stability.
- Cementing a liner into a stable cementless acetabular shell: the double-socket technique.
- biologic fixation:
- needs direct contact w/ host bone and osseointegration into the acetabular shell in order to provide long-term fixation;
- biologic fixation requires inherent stability of the implant;
- bone grafting of acetabular defects
- screw placement
- fixation w/ multiple acetabular screws enhances stability and minimally sacrifices the remaining bone;
- note that the quadrant system for safe screw insertion may not apply to a high hip center;
- screws are placed posterosuperiorly into the dome of the acetabulum and also inferiorly into the ischium;
- references:
- press fit cup at anatomic vs high hip center:
- press fit cup at a high hip center (>2 cm superior to the native hip center);
- medial protrusio technique
- rim fixation technique:
- jumbo press fit cup (66 to 80 mm)
- references:
- Revision of failed acetabular components with use of so-called jumbo noncemented components. A concise follow-up of a previous report.
- Treatment of large acetabular defects with jumbo cups.
- Acetabular revision arthroplasty using so-called jumbo cementless components: an average 7-year follow-up study.
- Jumbo cups and morsalized graft.
- Dealing with the deficient acetabulum in revision hip arthroplasty: the importance of implant migration and use of the jumbo cup.
- Jumbo cup or high hip center. Is bigger better?
- The fate of cementless jumbo cups in revision hip arthroplasty.
- Jumbo cups for revision of acetabular defects after total hip arthroplasty: a retrospective review of a case series
- references:
- oblong cup / modular cup-and-augment system:
- allows for less stripping of the ilium and less mobilization of the abductors;
- allows for faster and easier procedure;
- does not have the potential for resorption;
- note potential for debris generation at the interface, potential for fatigue failure, and inability to restore bone stock for future revisions;
- references:
- The use of bilobed porous-coated acetabular components without structural bone graft for type III acetabular defects in revision total hip arthroplasty: a prospective study with a minimum 2-year follow-up.
- Type III Acetabular Defect Revision With Bilobed Components: Five-Year Results
- Reconstruction of major segmental acetabular defects with an oblong-shaped cementless prosthesis: a long-term outcomes study.
- press fit hemispherical cup supported by structural allograft;
- bipolar arthroplasty:
gap cup and reconstruction rings »
femoral component considerations »
- even with isolated acetabular revision, have available selection of company appropriate femoral heads;
- revision of the acetabular component will involve additional reaming which will tend to further medialize the acetabulum, which means that re-insertion of the old modular femoral head will leave the hip loose and unstable;
- it is expected that a femoral head with a larger neck length will be required;
- in the case of residual instability, a 32 mm head (and appropriate liner should be available);
- references:
- Ten years of experience with porous acetabular components for revision surgery.
- Acetabular augmentation in primary and revision total hip arthroplasty with cementless prostheses.
- Revision Total Hip Arthroplasty with Cement after Cup Arthroplasty. Long-Term Follow-Up.
- Acetabular preparation in cementless revision total hip arthroplasty.
- Revision of the acetabulum without cement with use of the Harris-Galante porous-coated implant. Two to eight-year results.
- The Fate of Revised Uncemented Acetabular Components in Patients With Rheumatoid Arthritis.
- Cementless Acetabular Revision with the Harris-Galante Porous Prosthesis. Results After a Minimum of Ten Years of Follow-up.
- Revision of the acetabular component without cement after total hip arthroplasty. A concise follow-up, at fifteen to nineteen years, of a previous report.
Post Op Radiographic Evaluation »
Examples
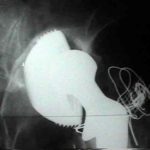
- example of an acetabular component that was obviously loose after 3 years;
- at surgery, the femoral component was secure and was left in place;
- the acetabulum was re-reamed for insertion of a larger component;
- a cortical allograft was anchored to the lateral femur inorder to re-oppose the abductors