
- See:
- Total Hip Replacement Menu:
- Acetabular Component Revision:
- Acetabular Defects Grafting Options: (frozen allograft)
- Dysplastic Hip:
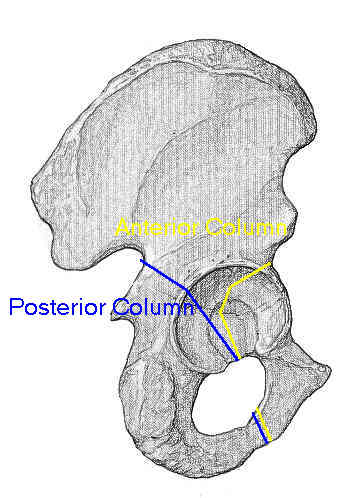
- Acetabular Radiographic Evaluation
- Posterior Column
- Discussion:
- based on the severity of bone loss and the ability to obtain cementless fixation for a given bone loss pattern;
- determines ability of remaining host bone to provide initial stability to a hemispherical cementless acetabular component until ingrowth occurs;
- classification based of integrity of: superior migration of the hip center, ischial osteolysis, acetabular teardrop osteolysis, and position of the
implant relative to the Kohler line:
- kohler line (ilioischial line): position of the implant relative to the Kohler line
- defined as a line connecting most lateral aspect of pelvic brim and most lateral aspect of obturator foramen on AP of pelvis;
- medial migration of the component relative to the Kohler line represents a deficiency of the anterior column;
- grade 1: medial aspect of the implant is lateral to the Kohler line;
- grade 2: there is migration to Kohler line or slight remodeling of iliopubic and ilioischial lines without a break in continuity;
- grade 3:
- migration medial to the line with Grade-3 migration;
- w/ extensive medial migration, consider angiography or CT w/ IV contrast and consider possible need for intrapelvic mobilization of vessels;
- osteolysis of teardrop:
- indicates bone loss from inferior and medial aspect of acetabulum, and inferior aspect of anterior column, lateral aspect of pubis, and medial wall;
- moderate osteolysis includes partial destruction of the structure with maintenance of the medial limb of the teardrop;
- severe involvement means complete obliteration of the teardrop;
- osteolysis of ischium:
- osteolysis is quantified by measuring distance from most inferior extent of lytic area to superior obturator line;
- indicates bone loss from the inferior aspect of the posterior column, including the posterior wall;
- acetabular component migration (superior migration of the hip center);
- superior migration is measured as the distance in millimeters (adjusted for magnification) relative to the superior obturator line;
- superior migration of the hip center represents bone loss in the acetabular dome involving the anterior and posterior columns;
- superior and medial migration indicates a greater involvement of the anterior column;
- superior and lateral migration indicates a greater involvement of the posterior column;
- Classifications:
- type I: rim is intact w/ no significant distortion of the rim
- acetabulum is hemispherical but there may be small focal areas of contained bone loss;
- anterior and posterior columns are intact;
- hemispherical cementless implant is almost completely supported by native bone and has full inherent stability;
- there is no migration of the component and no evidence of osteolysis in the ischium or teardrop;
- kohler line has not been violated (medialmost aspect of the component is lateral to the Kohler line);
- type II: distorted but intact rim with adequate remaining bone to support a hemispherical cementless implant;
- type IIa:
- anterior and posterior columns are supportive and the rim is intact
- bone loss is superior and medial;
- defect the hip center is migrated superior
- migration is less than 3 cm above the obturator line;
- failed component migrates into a cavitary defect medial to the thinned remaining superior rim;
- most defects are treated with particulate allograft because the defect is contained;
- type IIb:
- medial protrusio technique:
- anterior and posterior columns will support an implant but there is a small superior rim defect which is not contained;
- remaining anterior and posterior rims and columns are supportive for an implant;
- superior rim is deficient for less than one third of the rim circumferene;
- migration is less than 3 cm above the obturator line directly superior or in combination with lateral migration;
- femoral head allograft may be appropriate but majority of segmental defects are not grafted;
- particulate graft is not an option with the Type IIB defects because there is no buttress to contain the graft;
- type IIc:
- there is medial wall defects and migration of the component medial to Kohler's line;
- rim of the acetabulum is intact and will support the component;
- reconstructions involve particulate graft placed medially;
- if the medial membrane is not a sufficient buttress for the particulate graft, then insert a wafer of femoral head into the defect;
- graft is then placed over the wafer butress;
- type III:
- acetabular rim is not adequate for initial stability of the component;
- allograft is necessary to help restore deficient host bone (inorder to restore stability of the implant); (see acetabular allografting)
- posterior column may require reconstruction;
- type IIIa:
- characterized by greater than 3 cm of superior migration of the femoral component cephalad to the superior obturator line,
moderate teardrop and ischial lysis, and an intact Kohler line;
- host bone is adequate for ingrowth but the acetabular rim is not entirely supporative;
- defects are associated with a nonsupportive superior dome
- anterior and posterior columns remain intact, but hemispherical shell will have less than 50 percent host bone contact;
- migration of implant is superior and lateral;
- surgical options include: figure 7 shape distal femoral allograft, use of a bilobed implant or a trabecular metal acetabular component with a superiorly
placed trabecular metal augment, or cup placement in the high hip center;
- ref: Tantalum Augments for Paprosky IIIA Defects Remain Stable at Midterm Followup
- type IIIb:
- there is less than 40% of host bone available for ingrowth;
- rim defect is greater than 1/2 circumference;
- failed component has migrated superior and medial;
- high risk of occult pelvic discontinuity (posterior column reconstruction necessary)
- massive allografting and reconstruction cages are typically needed;
- references:
- Management of Severe Bone Loss in Acetabular Revision Using a Trabecular Metal Shell
- Treatment of type III acetabular deficiencies in revision total hip arthroplasty without structural bone-graft.
Classification and reconstruction in revision acetabular arthroplasty with bone stock deficiency.
Reliability of acetabular bone defect classification systems in revision total hip arthroplasty.
Principles of bone grafting in revision total hip arthroplasty: Acetabular technique.
Classification and reconstruction in revision acetabular arthroplasty with bone stock deficiency.
Management of massive acetabular defects in revision total hip arthroplasty.
Use of structural allografts in acetabular revision surgery.