

- Discussion:
- mechanism of injury:
- distinguish between high velocity injuries verus low velocity injuries (as this reflects incidence of vascular and nerve injuries);
- w/ low-velocity knee dislocations occurance of vascular injury is about 5% and nerve injury is about 20%
- references:
- Low-velocity knee dislocation.
- Beware of Ultra-Low-Velocity Knee Dislocation
- classification: 5 types: described w/ tibia in relation to femur;
- anterior (31%)
- occurs from hyperextension of knee (may need > 30 deg of hyperextension to produce this injury);
- often the PCL, & ACL will both be torn;
- either the MCL or LCL or both will usually be injured;
- alternatively, hyper-extension injuries may cause disruption of the ACL and posterior capsule while the PCL is spared;
- popliteal artery is tethered proximally at adductor hiatus & distally by arch of soleus;
- injury to the popliteal artery may initially manifest as an intimal tear or intraluminal thrombus (damage is over a longer segment of the artery);

- posterior (25%)
- there is disruption of both cruciate ligaments
- possible extensor mechanism disruption;
- avulsion of or complete disruption of of popliteal artery depending on magnitude of injury
- more likely to produce localized injury (isolated transection);
- lateral (13%)
- medial (3%)
- rotary (4% - usually posterolateral)
- references:
- Complete dislocation of the knee without disruption of both cruciate ligaments.
- Complete knee dislocation without posterior cruciate ligament disruption. A report of four cases and review of the literature.
- Posterior dislocation of total knee arthroplasty.
- Knee dislocations with intact PCL.
- Knee dislocations: where are the lesions? A prospective evaluation of surgical findings in 63 cases.
- Clinical Findings:
- note the frequent occurence that the closed reduction will be performed by EMS, and so the diagnosis at first glance may not be obvious;
- note the occurrence of an LCL ligament disruption + peroneal nerve palsy = knee dislocation;
- popliteal artery & vein injury is common; (see management of vascular injuries)
- its important to note that knee dilocations that have spontaneously reduced may look benign but may lead to thrombosis of the popliteal artery.
- peroneal nerve injury:
- occurs in 20% to 40% of knee dislocations & approximately half of these palsies are permanent;
- note that apparent neurologic injury may in many cases be due to ischemia;
- typically both cruciates and least one collateral ligament are disrupted;
- w/ peroneal nerve injury, be highly suspect for vascular injury;
- even if pulse returns following reduction, consider need for arteriogram, since incidence of intimal injury is high w/ concomitant nerve injury;
- reference:
- Palsy of the common peroneal nerve after traumatic dislocation of the knee.
- assessment of ligament injuries:
- at the earliest opportunity, the patient should have an examination under anesthesia;
- this can often be performed during vascular repair or during anesthesia for management of other injuries (abdominal exploration ect);
- this allows clinical determination of the ACL, PCL, LCL, Posterolateral corner, and MCL;
- ref: Examination of the patient with a knee dislocation. The case for selective arteriography.

 - Radiographs:
- Radiographs: - associated radiographic findings:
- tibial plateau frx dislocations:
- proximal fibular frx
- avulsion frx of gerdey's tubercle;
- intercondylar spine frx
- avulsion of fibular head;
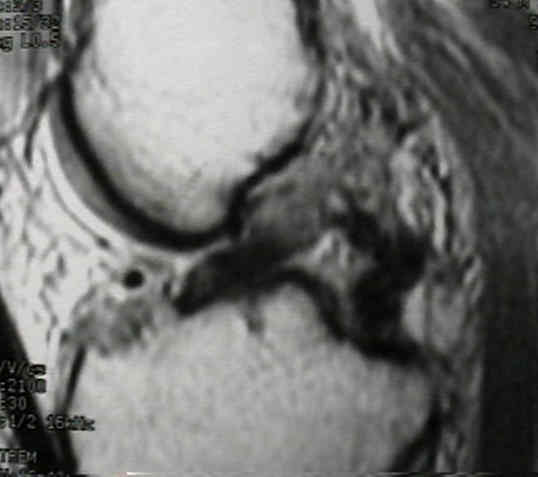
- MRI:
- MRI not only allows assessment of which ligments are intact but also helps determine whether ligament tears are midsubstance or are avulsions (off the femur or tibia);


- Management of Knee Dislocations:
- closed reduction:
- closed reduction is performed as soon as possible (with follow vascular checks);
- note that reduction may be complicated by interposed soft tissue;
- subluxation or recurrent dislocation is common;
- immobilize the reduced knee in approximately 20? of flexion with hinged knee brace;
- avoid placing in too much extension, since the lax posterior capsule permits subluxation;
- if adequate reduction is possible but cannot be maintained, then consider external fixation;
- it is important that the external fixator pin sites will not interfere with the ACL/PCL tunnel sites (during future ligament reconstruction);
- ref: Two cases of irreducible knee dislocation occurring simultaneously in two patients and a review of the literature.
- management of vascular injuries in knee dislocation:
- expectation is that vascular surgery and compartment fascial release is required;
- if pulses are completely normal and symmetric, normal neurological exam, and soft compartments, then in hospital observation is accetable;
- compartment syndrome:
- compartment syndrome is a frequent complication of knee dislocation, attributable to vascular injury and resultant ischemia;
- four compartment fasciotomy is indicated in these situations;
- nerve injury:
- peroneal nerve is often disrupted w/ concomitant LCL injuries, but in some cases there will be tibial nerve injury as well;
- one of problems encountered in peroneal nerve repair following knee dislocations (or other injuries) is that location of nerve injury may be well above knee joint;
- in the case of knee dislocation, there may be concomitant tibial nerve division palsy;
- hence, it should not be assumed that nerve repair (or nerve jump graft) will be possible using a standard posterolateral incision;
- Treatment of Ligament Injuries:
- timing:
- if vascular injury has been previously repaired, get clearance from the vascular surgeon to utilize a tourniquet;
- in cases of intimal flap tears, a loading dose of intravenous heparin is given before tourniquet inflation inorder to minimize the risk of thrombus formation;
- for patients that have had an arterial repair, most authors tend to wait two weeks to assure vessel patency;
- primary repair:
- PCL avulsions
- often the PCL (and sometimes the ACL) will be avulsed from either the femoral or tibial attachement;
- in these cases the ligament can be re-attached using a "suture - pull thru" technique;
- the ACL tibial guide will faciliate accurate assessment of pull thru drill holes;
- in some cases the anterolateral bundle is ruptured but the posteromedial bundle and meniscofemoral ligament is intact;
- references:
- Primary repair of knee dislocations: results in 25 patients (28 knees) at a mean follow-up of four years.
- Re: primary repair of knee dislocations: results in 25 patients (28 knees) at a mean follow-up of four years.
- Comparison of Surgical Repair or Reconstruction of the Cruciate Ligaments versus Nonsurgical Treatment in Patients with Traumatic Knee Dislocations
- reconstruction:
- surgical reconstruction sequentially adresses ligament tears determined from clinical exam, MRI, and/or arthroscopy (the later may cause
compartment syndrome due to capsular disruption);
- common instability patterns include the ACL/PCL with either the MCL or LCL injured as well;
- often the PCL (and sometimes the ACL) will be avulsed from either the femoral or tibial attachement;
- in these cases the ligament can be re-attached using a "suture - pull thru" technique;
- the ACL tibial guide will faciliate accurate assessment of pull thru drill holes;
- note that reconstructing the ACL without repairing or reconstructing the PCL can result in a posteriorly displaced tibia;
- allografts (bone-patella-bone or Achilles tendon) should be available;
- ref: Dynamic intraligamentary stabilization and primary repair: A new concept for the treatment of knee dislocation.
- other considerations:
- Hinged External Fixation in the Treatment of Knee Dislocations: A Prospective Randomized Study
- Is Stability of the Proximal Tibiofibular Joint Important in the Multiligament-injured Knee?
- postoperative management:
- early ROM is encouraged to avoid the complication of knee stiffness;
- references:
- Comparison of Surgical Repair or Reconstruction of the Cruciate Ligaments versus Nonsurgical Treatment in Patients with Traumatic Knee Dislocations
- Results after treatment of traumatic knee dislocations: a report of 26 cases.
- Does Sequence of Graft Tensioning Affect Outcomes in Combined Anterior and Posterior Cruciate Ligament Reconstructions?
Traumatic dislocation of the knee joint.
Traumatic dislocation of the knee.
Dislocation of the knee.
Femoral-sided fracture-dislocation of the knee.
Surgical Management of Knee Dislocations.