
- See:
- Bone Grafting for Tibial Fracture / Management of Tibial Bone Defects
- Tibial Non Unions / Infected Non Unions
- Discussion:
- used most in middle and distal third fractures;
- posterolateral bone grafting may be used for infected non-unions & is performed w/o disturbing anteromedial soft tissue which often bear brunt of soft tissue injury;
- whenever possible to avoid further surgical dissection to a previously traumatized area;
- anterior soft tissue damage precludes anterior operative approach;
- posterolateral graft via virgin approach is often best choice;
- w/ massive bone loss, posterolateral bone grafting obtains fracture stability by creating a tibio-fibular synostosis above and below the frx site;
- average time to union w/ posterolateral bone grafting is about 5 months;
- as might be expected, time to union is quicker w/ bone grafting performed w/ in 6-8 weeks of injury;
- some authors advocate early grafting for all high energy tibial fractures;
- advantages:
- allows a virgin approach to be used which avoids subjecting previously traumatized area to more insult;
- useful for treating infected non unions & can be performed w/o disturbing anteromedial soft tissue defects;
- allows a large amount of cancellous bone graft to be applied;
- Relative Contra-Indications:
- previous fibulectomy which will comprimise the synostosis above and below the frx site;
- proximal third fractures: higher risk of neurovascular injury;
- drainage from front of leg may not be a contra-indication to grafting by post-lateral approach if fibrous barrier across frx undisturbed;
- the surgical approach for the graft placement should not pass thru an active or recently infected area;
- Anatomy:
- Anterior Compartment
- Lateral Compartment
- Deep Posterior Compartment:
- Superfical Posterior
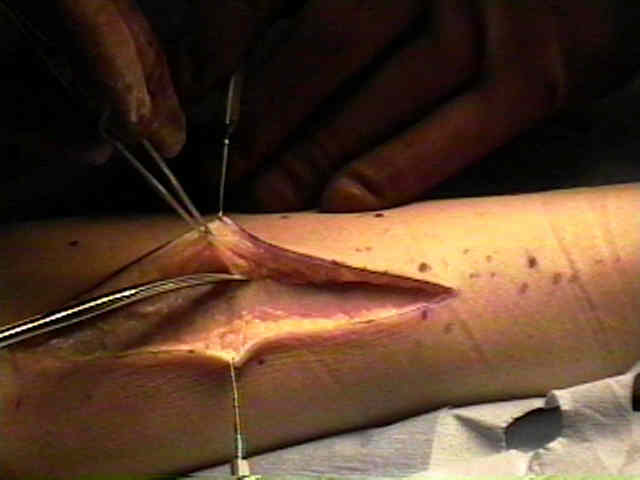
- Technique:
- patient is placed in the lateral position;
- consider obtaining a both a preoperative and postoperative 35 deg internal oblique view of the tibia, to better view the defect;
- incision is made just posterior to the fibula to allow 5 cm of exposure above and below the frx;
- posterolateral approach to tibia:
- cutaneous branch of the peroneal nerve is protected;
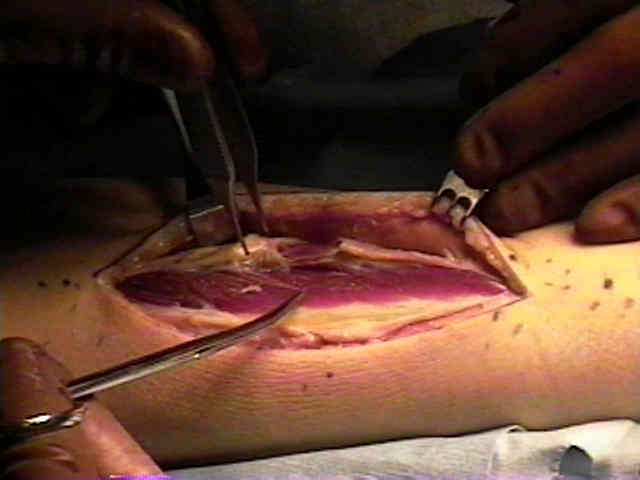
- access to posterior compartment lies between peroneal and posterior compartment muscle masses;
- the interosseous membrane should not be violated;
- w/ moderate bone loss, the posterior tibial surface is roughened above and below the frx surface, and then crest bone graft is placed over the fracture site;
- a tibio-fibular synostosis is note required;
- see: bone graft harvest technique:
- w/ major bone loss, then bone graft should be carried to fibula (considered to be a salvage procedure);
- it may not necessary to disturb the fibrous union at the frx site since bony stability is obtained by the synostosis;
- stability will be obtained from the synostosis above and below the frx site;
- osteoperiosteal flaps can be raised from the fibula to posterior aspect of the tibia proximal and distal to the fracture site;
- crest bone graft is then added to create the synostosis;
- patients should be warned of possible ankle problems following synostosis;
- at wound closure, the deep fascia is not closed;
- Case Example:
- 25 yr old who sustained high velocity type II segmental open tibia frx;
- at 8 weeks there are some signs of healing, but there is at least a 50% cortical defect on both the AP and lateral views;
- the indications for bone grafting here include: high velocity, segmental fracture, w/ significant cortical defect




- technique: 

Posterior bone grafting of the tibial for nonunion: a review of twenty-four cases.
A simplified surgical approach to the posterior tibia for bone grafting and fibular transference.
The value of internal oblique radiographs for posterolateral bone grafting of the tibia.
Posterolateral bone graft of the tibia.
Treatment of infected nonunion of the tibia through the posterolateral approach.
Posterolateral bone graft for nonunion of the tibia.
The value of posterolateral bone-grafting for non-union of the tibia.
Original Text by Clifford R. Wheeless, III, MD.
Last updated by Clifford R. Wheeless, III, MD on Friday, February 15, 2013 4:05 pm