
- See: MP joint in RA
- Planning:
- indications:
- irretrievable articular cartilage damage;
- volar subluxation;
- dislocation are indications for surgery;
- cautions:
- cervical spine in RA;
- wrist disease:
- healthy axiom for surgery in RA is to start proximally & work distally alternating fusion with motion sparing procedures;
- hence consider adressing wrist disease before MP disease;
- MP arthroplasty is generally performed only after wrist alignment has been reestablished;
- w/ correctable radial deviation deformity, consider tendon transfer ECRL, to the ECU tendon;
- extensor tendon rupture:
- arises from RU instability and caput instability syndrome;
- tendon repair & synovectomy of tendon sheaths may procede or follow MP arthroplasty;
- w/ extensor tendons rupture & MP joint dislocation, arthroplasty of MP joints are done before wrist & tendon reconstruction;
- flexor tendon rupture:
- MP joint arthroplasty should not be performed until flexor tendons have been reconstructed;
- goals: arthroplasty should provide the following:
- pain relief
- ulnar drift improvement (from 25 deg to 5 deg)
- extension deficit improvement (from 56 deg to 10 deg)
- don't expect increase in strength;
- concomitant PIP deformity:
- if PIP joints are stiff in extension, then consider a preoperative hand therapy for PIP ROM excercises;
- often a surprising amount of PIP ROM can be gained which will facilitate postoperative rehab;
- w/ swan neck deformity, MP & PIP joints are reconsturcted at same stage;
- w/ a boutonniere deformity, PIP is reconstructed first;
- tendon imbalances and joint malalignment must be corrected;
- implant arthroplasty for both the MP and PIP joints of the same digit is usually not recommended;
- severe deformity of both MCP & IP joints of thumb w/ intact CMC joint is indication for arthrodesis of both MCP & IP joints;
- equipment:
- ensure that proper sizes of the implants are available (often the index, long, and ring fingers will take the same size and the little finger will take a smaller size (therefore there needs to be at least three of each size);
- motorized burr, homan retractors, skin hooks, several 15 blade scaples;
- technique considerations:
- procedure is best performed with two surgeons (the surgeon on one side of the table is positioned to perform the phalangeal broaching and the other surgeon is positioned to perform the metacarpal broaching);
- correct wrist deformity first if necessary
- soft tissue releases as necessary
- intrinsic tendon release
- extensor tendon relocation
- reconstruction of radial side collateral ligament
- postoperative spinting and hand therapy;
- Surgical Technique:

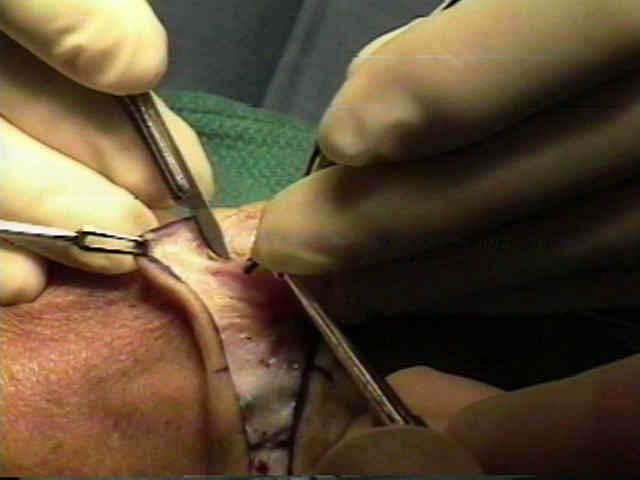
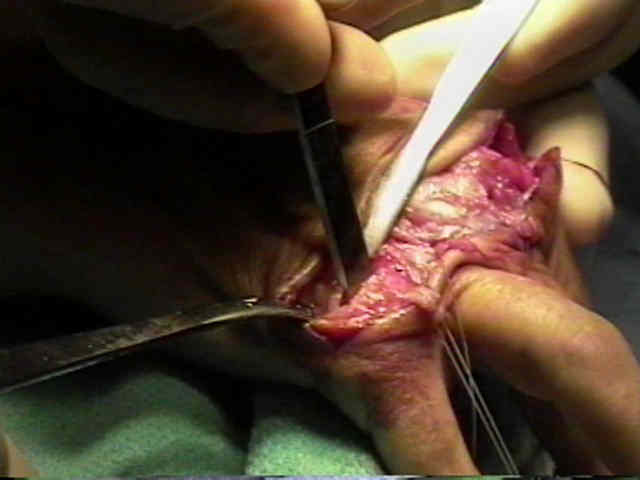
- surgical approach:
- transverse incision over necks of metacarpals to expose extensor tendons;
- superficial veins and nerves preserved (these often lie between the metacarpals);
- note whether ulnar subluxation or rupture of the extensor tendons is present;
- bluntly separate the extensor mechanism from the underlying joint capsule;
- saggital band release:
- in the long, and ring fingers, mid aspect of the saggital band is transected on both sides of the extensor tendon;
- in the index and little fingers, ulnar sided incision made between EDC and extensor digiti minimi tendons, in addition to the radial sided incision through the mid aspect of the saggital band;
- intrinsic tendon release:
- ulnar sided intrinsic tendons can be released at this stage in the procedure or may be released later in the case by stripping the ulnar collateral ligament off of the proximal phalanx along with the intrinsic tendon;
- obviously, release of intrinsics will disrupt their normal function (MCP flexion and digit extension);
- index finger: some surgeons will avoid releasing the intrinsic tendon off of the index finger because it provides a pronating force (which is essential to pinch);
- little finger:
- in little finger, ADQ tendon is divided;
- flexor digiti minimi brevis tendon preserved;
- in ring and little finger, release of the ulnar intrinsics may cause significant loss of active flexor power at the MCP joints;
- capsular release:
- since volar phalangeal dislocation is usually present, this dissection is usually easier once the metacarpal neck has been transected;
- joint capsule is elvated on both sides of the metacarpal, and on the ulnar side of the proximal phalanx;
- ulnar sided stripping should release the ulnar collateral as well as the phalangeal insertion of the intrinsic muscle;
- if reduction of the MP joint is difficult, then strip the ulnar half of the volar plate;
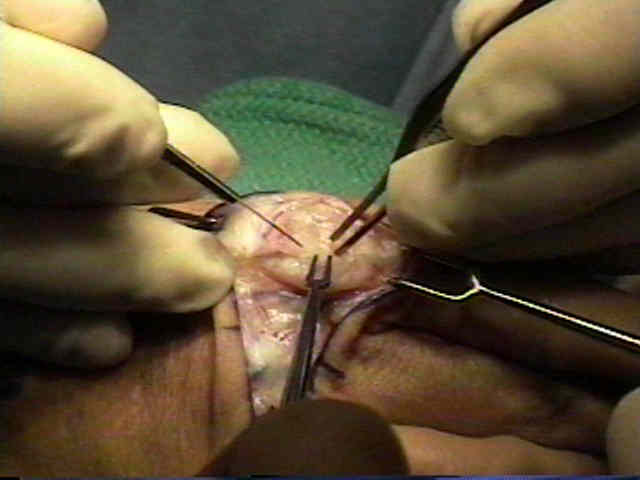
- metacarpal neck resection:
- sharply elevate the collateral ligaments off of the metacarpal neck;
- once exposure is optimal, use an saw to transect the MP heads (at the neck);
- two small homan retractors are placed beneath the metacarpal neck;
- head of metacarpal resected, and part of flare of metaphysis preserved;
- it is better to underresect than overresect because overresection may make the metacarpal-phalangeal interval too wide, which will leave the prosthesis loose and prone to dislocations);
- bone ends are smoothed;
- synovectomy and soft tissue release completed;
- do not broach the metacarpal at this point (broach the proximal phalanages first because this is usually the limiting factor for stem size);
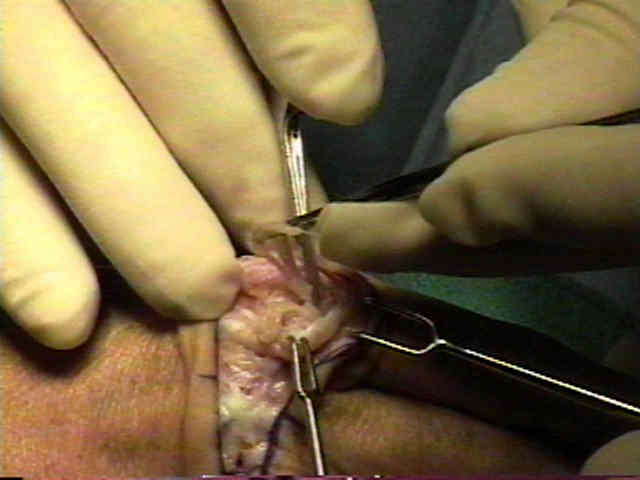
- proximal phalangeal preparation:
- ensure that adequate soft tissue release and exposure of the proximal phalanx has been performed (release the volar plate if necessary for proper exposure);
- when broaching the medullary canal the surgeon should hold the proximal phalanx in one hand and broach with the other;
- the hand holding the phalanx helps the surgeon "sense" the position of the phalanx and helps broaching;
- use a motorized burr to enter the medullary canal of the proximal phalanx;
- begin broaching and attempt to use the largest broach as possible;
- index finger: because the index finger needs to be positioned in slight pronation (for pinch), proximal phalangeal broaching needs to be performed slightly asymmetrically (dorsal ulnar to palmar radial direction);
- metacarpal broaching:
- the surgeon should grasp the metacarpal in one hand and broach with the other;
- broaching is carried out upto the size achieved for the proximal phalanx;
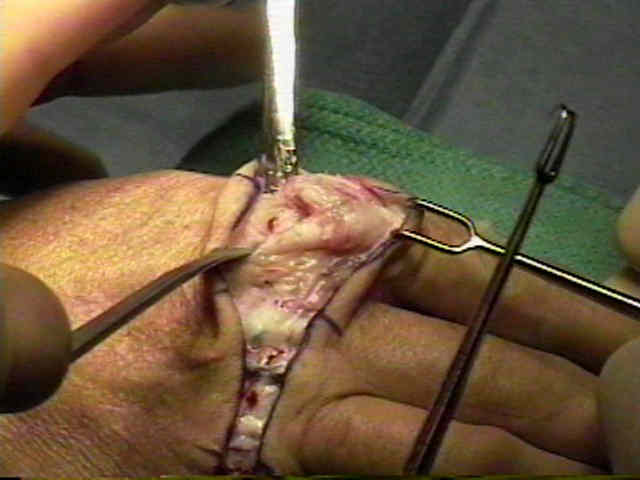
- implant insertion:
- the surgeon should wash all talc off of his/her gloves before handling the implant;
- insert implant and be sure that there is sufficient space so that there is no implant buckling;
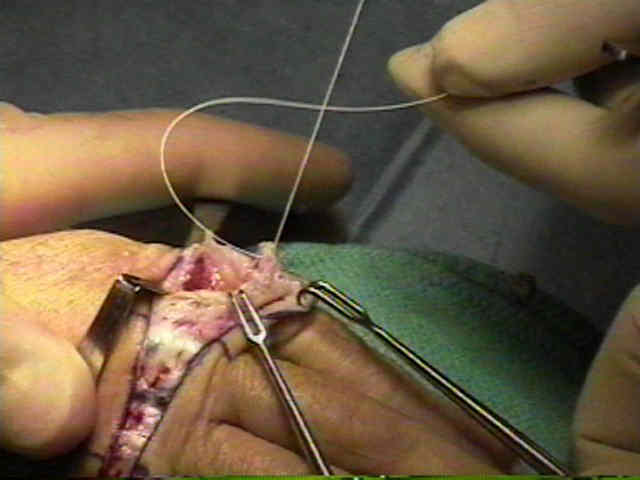
- closure:
- secure the capsular flaps with horizontal matress sutures (goal is to cover implant - decreasing risk of infection);
- in some cases radial collateral ligament reefing may be necessary (this may incorporate the radial half of the volar plate);
- crossed intrinsic transfer:
- in the report by Pereira, et al, 43 hands in 36 adults undergoing Silastic interposition arthroplasty of the index, middle, ring and little finger MP joints for RA were randomly allocated to undergo replacement with or without crossed intrinsic transfer;
- pre-operative clinical measurements of the two groups were indistinguishable;
- both groups showed improvement in ulnar drift and an altered arc, but no change in total range of motion at the MP joints;
- grip strength and pulp to pulp pinch were significantly and comparably improved in both groups;
- it is concluded that crossed intrinsic transfer does not significantly affect the outcome of Silastic interposition arthroplasty of the metacarpophalangeal joints in rheumatoid patients;
- ref: A comparison of metacarpophalangeal joint silastic arthroplasty with or without crossed intrisic transfer.
- extensor tendon realignment:
- radial realignment of the extensor tendon helps control ulnar deviation of the digits;
- unfortunately the ulnar deviation of the flexor tendons cannot be addressed through the dorsal incision;
- sagittal fibers of dorsal hood reefed in overlapping fashion on radial side to centralize long extensor tendon and maintain correction;
- previously incised junctura may be repaired as long as they do not interfere with tendon centralization;
- Post Operative Care:
- static forearm splint: (for 12 weeks of night use)
- wrist is maintained in 20 deg of extension (if possible);
- MP joints are placed in near full extension and slight radial deviation;
- dorsal splint with dynamic outrigger (modified Madden protocol);
- same position as the static forearm splint;
- patients should perform 10 repetitions q 2 hrs for a total arc of motion from full extension to maximal tolerated flexion;
- active and passive extension and flexion of the IP joints are performed for ten repetitions q 2 hours;
- at 6 weeks the dynamic splint is discontinued;
- patients need to avoid key pinch for the first 12 weeks postop;
- at two weeks, the patient is encouraged to begin "radial walking" (active finger radial deviation);
- at six weeks the patient is given soft putty for hand strengthening;
- Complications:
- recurrent ulnar drift:
- prevented by prolonged postoperative dynamic splinting;
- lack of MP joint extension:
- maldirection of the bone cuts;
- excessive bony resection;
- flexor adhesion;
- synovitis or triggering of flexor tendons;
- extensor tendon rupture or subluxation
- radial nerve entrapment;
- prosthesis fracture:
- silicone synovitis: uncommon in the MP and PIP joints (but is common in the carpi);
- infection: rare in the MP joints;
- persistent volar subluxation of the proximal phalanx: Harrison Sling
- 4 cm slip of extensor tendon 5 mm wide is detached proximally and freed distally to the distal portion of the MCP joint;
- this is passed through a drill hole made in the dorsal cortex of the proximal phalanx;
- tendon is passed thru the drill hole and is sutured back on itself;
- this provides a strong extensor force holding the base of proximal phalanx in its relocated position;
- Outcomes:
- in the report by McGovern RM, et al, the authors performed a retrospective evaluation of the Steffee MCP thumb joint prostheses;
- 54 primary thumb arthroplasties (49 patients) were performed for pain, weakness, or instability involving the thumb MCP joint secondary to arthritis;
- 31 thumbs had concomitant IP joint instability and underwent IP joint fusions;
- at an average follow-up period of 57 months, the average motion of the MCP joint was 21° (range, 0° to 40°), with a significant improvement in position and stability;
- although there was not a consistent long-term improvement in grip or pinch strength, 87% of the patients reported subjective improvement in strength and function as a result of surgery;
- pain was relieved in all thumbs with preoperative pain;
- complications included a periprosthetic fracture, 2 late infections, and 1 gross loosening of the implant;
- survivorship of the implant was 93% survivorship at 5 years and 89% survivorship at 10 years, with only 4 failures in 54 thumbs;
- Steffee thumb MCP arthroplasty resulted in excellent long-term survivorship, patient satisfaction, and functional outcome;
- ref: Long-term results of cemented Steffee arthroplasty of the thumb metacarpophalangeal joint.
- Case Example:















A rational postoperative management program for metacarpophalangeal joint implant arthroplasty.
Silastic arthroplasty in rheumatoid MCP-joints.
Flexible (silicone) implant arthroplasty of the metacarpophalangeal joint of the thumb.
Silicone-rubber implant arthroplasty of the metacarpophalangeal joints for rheumatoid arthritis.
Metacarpophalangeal joint implant arthroplasty with a Silastic spacer.
Silicone-rubber implant arthroplasty of the metacarpophalangeal joints for rheumatoid arthritis.
Metacarpophalangeal Joint Arthroplasty in Rheumatoid Arthritis.