
- Discussion:
- characterized by frx of volar margin of the carpal surface of the radius which is associated w/ subluxation of radiocarpal joint;
- similar to Smith's type III;
- comminuted frx of distal radius may involve either anterior or posterior cortex and may extend into the wrist joint;
- both involve volar dislocation of carpus assoc w/ intra articular distal radius component;
- frx dislocation or subluxation in which the rim of distal radius, dorsally or volarly is displaced with the hand and carpus;
- it differs from Colles' or Smith's Fracture in that the dislocation is the most striking radiographic finding;
- volar Barton's is more common than dorsal Barton frxs;
- mechanism:
- usually result from a fall upon an outstretched arm, leading to dorsiflexion stress and tension failure of volar lip of radius;
- strong volar radiocarpal ligaments avulse the volar lip of the radius from the metaphysis;

- Radiographs:
- frx cleft extends proximally in coronal plane in oblique direction, so that free fragment is wedge shaped;
- carpus is displaced volarly & proximally w/ articular fragment;
- w/ volar Barton's frx, it is critical to note whether there is more ulnar or radial sided comminution
(since this will affect the choice of surgical approach);
- if necessary, order a CT scan to better define the anatomy;
- Non Operative Treatment:
- most of these fractures will require operative treatment;
- if non operative treatment is attempt, be sure to immobilize the wrist palmar flexed which will tip the carpi away from the
fractured volar surface;
- ORIF and Surgical Approach for Anteriorly Displaced Frx:
- ORIF is required for all displaced volar articular lip fractures;
- even with initial acceptable reduction (w/ wrist in extension), recurrance of palmar subluxation is common;
- strong proximal pull of the extrinsic wrist and digital flexors and extensors makes closed reduction difficult and predisposes joint
to redisplacement;
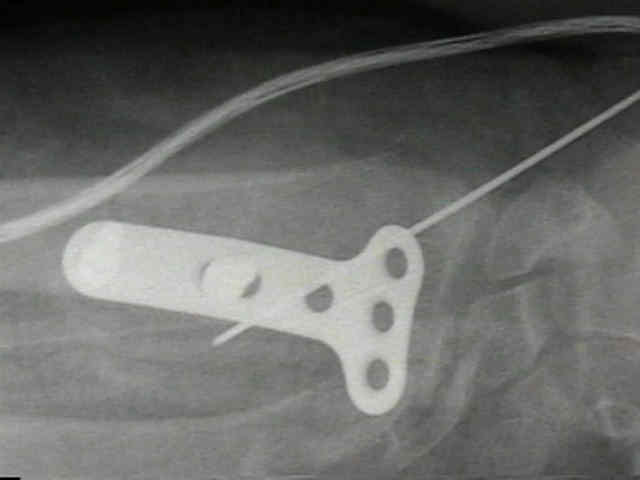
- implants:
- volar plates are well tolerated, and seldom need to be removed;
- small T plate on the volar aspect;
- plate is bent in mid portion to effect prebending effect;
- ensure that the distal margin of the plate does not encroach on the articular surface (using flouro);
- slight dorsal articular penetration may be allowable;
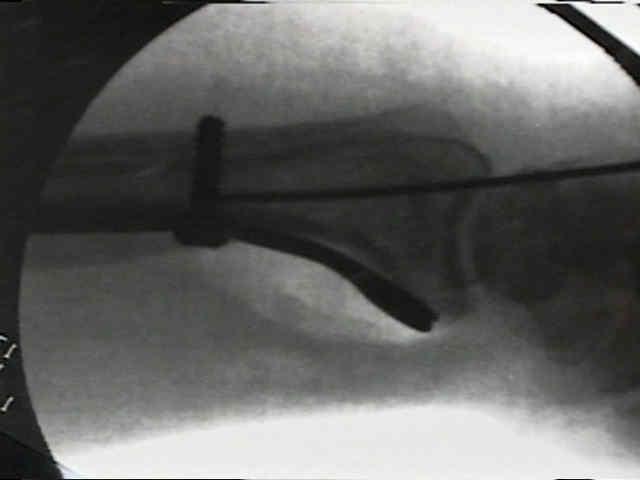
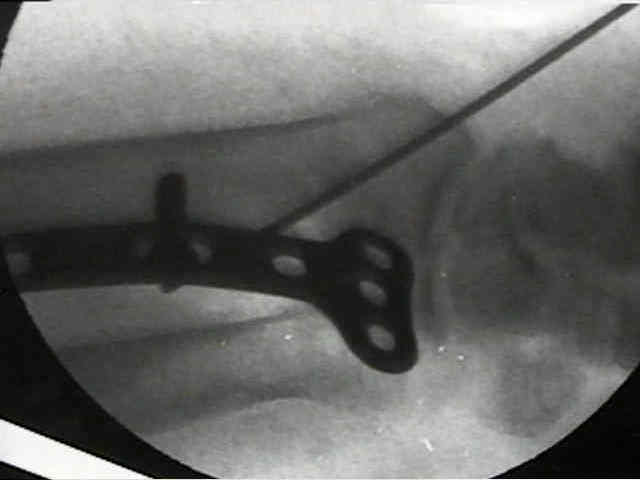
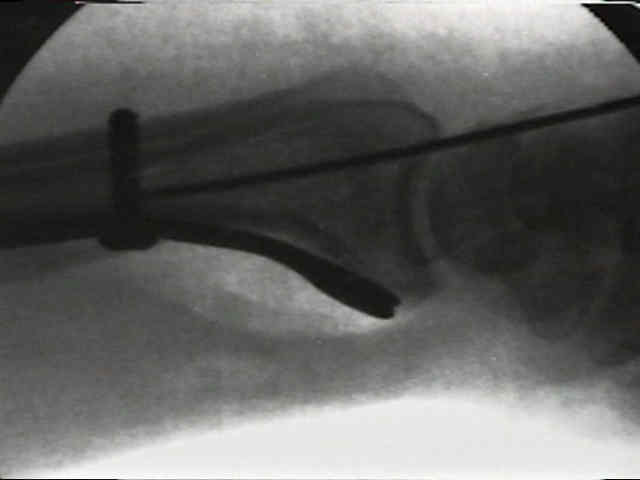
- begin w/ a proximal screw (3.5 cortical) placed into the distal side of the oval hole, which will have the effect of moving the
plate distally (which then applies compression to the periarticular fragments);
- subsequently, insert the distal screw (4.0 cancellous) only if it is needed










Barton's Fractures.
Anterior and posterior marginal fracture-dislocations of the distal radius. An analysis of the results of treatment.
Barton's fractures - reverse Barton's fracture. Confusing eponyms.
Volar barton’s fractures with concomitant dorsal fracture in older patients.