
- Treatment Options:
- No Reduction - elevation, compression, early ROM (ROWE)
- Closed Reduction - Bohler: distraction/M-L - compression
- Open Reduction
- Palmer: lateral approach (1948)
- Goals of Open Reduction:
- restore anatomy, artiuclar surface, ht/width, varus/valgus;
- Non Operative Treatment:
- most crucial measurement is degree of continuity of posterior facet, which is best determined by CT scan;
- all frx are initially treated by strict bed rest, elevation, until acute swelling has subsided;
- early mobilization with protection from wt bearing until frx union occurs;
- nondisplaced frx w/ mild or moderate decrease in Bohler's < are initially treated by early mobilization, avoidance of wt bearing for 6 weeks;
- may need to be supplemented by orthotic support with a custom-molded insole, rocker-bottom shoe, or ankle-foot orthosis;
- when nonoperative treatment fails, sub-talar arthrodesis is often indicated;
- Management of Associated Injuries:
- compartment syndrome
- deep central compartment is involved most often in calcaneal frx;
- ref: Compartment syndrome of the foot after intraarticular calcaneal fracture.
- management of soft tissues and frx blisters:
- note: if surgery is to be delayed inorder to allow swelling or frx blisters to subside then ensure that an adequate closed reduction has been achieved so that displaced frx fragments do not tent the soft tissues;
- on occassion a patient's splint will be removed only to find that there is soft tissue necrosis from displaced frx fragments;
- timing of surgery:
- realizing that mechanism usually invovles direct trauma to the heel, it is no surprise that contusion, hemorrhage, and swelling are common;
- because of soft tissue contussion, there has be a general trend to delay surgery 7-10 days;
- patients should be maintained w/ gentle compression wrap, and strict leg elevation; 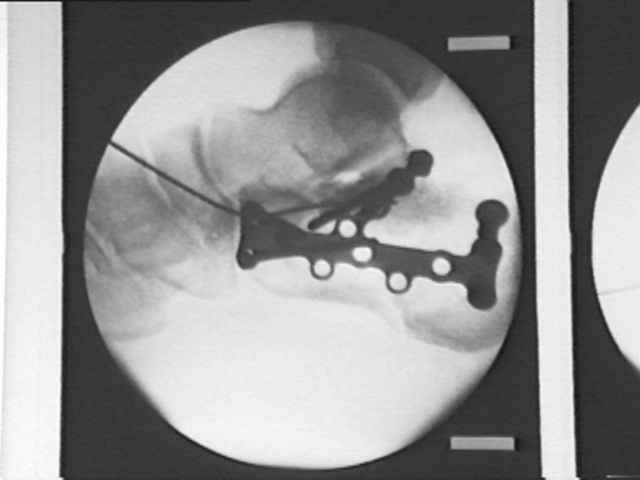
- ref:
The management of soft-tissue problems associated with calcaneal fractures.
- Operative Treatment:
- implants:
- 3.5 mm cortex or cannulated screws, or 4.5 mm cannulated screws as lag screws (medial fragment including sustentaculum tali);
- be aware that bicortical fixation of the medial fragment has a high risk of injurying the FHL, nerves, and vessels;
- alterantively consider use of 4.0 cancellous screws rather than bicortical 3.5 mm cortical screws (even for fixation of the medial fragment);
- as pointed out by Bailey, et al., 4.0 mm cancellous screws provided just as good fixation as 3.5 cortical screws since mechanical failure will occur thru ligament disruption rather than screw pullout;
- 3.5 mm reconstruction plate, Synthes 3.5 mm calcaneal plates, or a flattened 3.5 mm 1/3 tubular plate;
- as noted by Carr, et al in an cadaveric model, the flattened 1/3 tubular plate had a similar load to failure as compared to a 3.5 mm recon plate;
- they concluded that the lower profile 1/3 tubular plate would be a better choice inorder to avoid wound healing complications;
- Intraarticular calcaneus fractures: a biomechanical comparison or two fixation methods.
- Internal fixation of experimental intra-articular calcaneal fractures: a biomechanical analysis of two fixation methods.
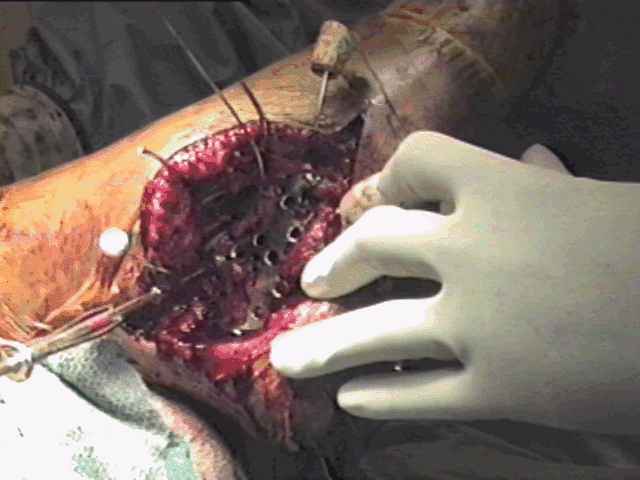
- lateral approach and surgical fixation:
- pt in true lateral position
- J or L approach w/ subperiosteal dissection off lateral wall, including calcaneo-fibular ligament (sural nerve in flap)
- extension from tuberosity to calcaneo-cuboid (watch peroneals)
- addresses lateral wall (width)
- calcaneo-cuboid joint / posterior facet facet;
- restoration of height and tuber alignment
- indirect tuber --> sustentaculum reduction;
- reduction of critical angle of Gissane/ anterior process to sustentacular fragment;
- reduction of posterior facet;
- reduction of tuberostiy/lateral wall last - x-rays to confirm reduction;
- bone graft cancellous defects (optional);
- fixation (see below);
- 1/8 in hemavac;
- early ROM, non wt bearing 10-12 weeks, hardware out = 1 year;
- Post Op:
- regardless of type of treatment most authors recommend avoidance of wt bearing for 8 to 12 weeks following fracture;
- working person can often return to work at 4-6 months with an AFO;
- Primary Fusion: (see: sub-talar arthrodesis)
- indicated for fractures w/ more than 3 parts;
- restores length of gastrocnemius-soleus complex
- corrects flat foot
- relieves the narrow peroneal space;
- surgical stratedgy:
- restore anatomy as would be performed w/ ORIF;
- expose sinus tarsi as would typically be performed for subtalar fusion;
- currette or burr out the posterior facet;
- apply iliac crest bone graft to obtain both an intra- and extra-articular arthrodesis;
- Fully Threaded 7 mm Cannulated Screw:
- guide pin is inserted in postero-inferior aspect of tuberosity fragment and is driven up into talar neck;
- avoid inserting pin into lateral fragment;
- an ACL "tibial tunnel guide" may be helpful for positioning the pin
Intraarticular calcaneus fractures: a biomechanical comparison or two fixation methods.
Surgical management of fractures of the os calcis.
Operative treatment of intra-articular fractures of the calcaneus.
Fractures of the calcaneum: the anterolateral fragment.
Operative treatment of displaced intra-articular fractures of the calcaneum. Medium-term results.
Osteosynthesis of displaced intraarticular fractures of the calcaneus. Results in 123 cases.
Open treatment of acute calcaneal fractures.
Intraarticular calcaneal fractures. Results of closed treatment.
Open reduction and circular external fixation of intraarticular calcaneal fractures.
Surgical management of calcaneal fractures using bilateral incisions and minimal internal fixation.
Extensive intraarticular fractures of the foot. Surgical management of calcaneal fractures.