- Discussion:
- indications for patellar resurfacing
- patellar malalignment
- lateral retinacular release
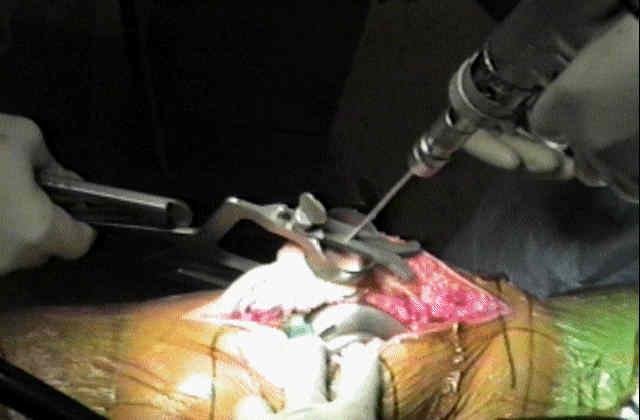
- Technique:
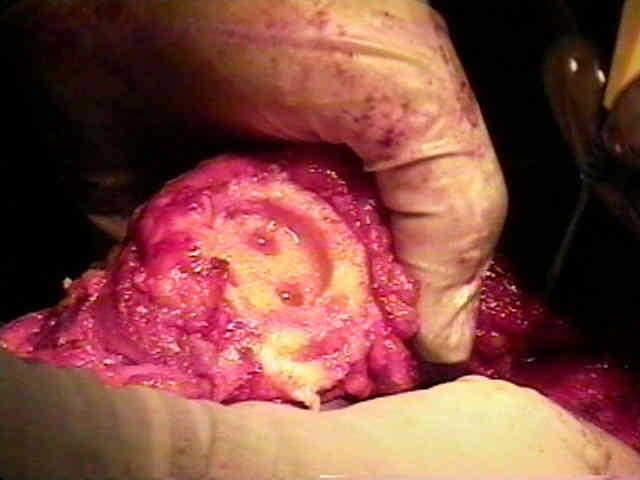
- start by everting the patella laterally and reflecting the fat pad & synovium from around its periphery;
- remove any overhanging osteophytes;
- limited patellar fasciectomy should be a part of every resurfacing (to avoid lateral patellofemoral impingement)
- note propensity for subluxatation: (see patellar subluxation));
- prior to pataller resurfacing take the knee through several ROM and note whether subluxation is present;
- if subluxation is present (and tibial component is properly rotated), then patellar component should be medialized as much as possible (to minimize subluxation);
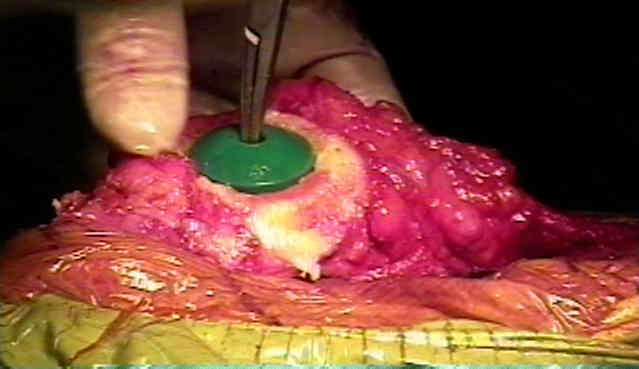
- determine geometric center: (see patellar anatomy);
- align geometric center of prosthetic patellar implant w/ geometric center of patella (not w/ central ridge, which is medial to geometric center);
- this ridge orients the longitudinal axis of the patella;
- in cases of pre-existing propensity for patellar subluxation, the central point of reaming should be moved medially;
- pitfalls: asymmetric resurfacing
- in some cases the medial patellar facet will be overgrown by synovium or will be eroded by arthrosis;
- do not confuse the lateral patellar facet for the main patellar surface;
- use the cautery to carefully demarcate the medial and lateral articular borders of the patellar facet;
- in the report by Pagnano, et al, 300 consecutive TKAs were reviewed for presence of asymmetric patella resurfacing using a postop Merchant view;
- 21 knees in 14 patients were found to have the patella asymmetrically resurfaced;
- asymmetric resurfacing typically involved inadvertent excessive resurfacing of lateral facet w/ underresection of bone from medial patellar facet;
- all patients underwent follow-up for a minimum of 5 years, with a mean follow-up of 7.5 years;
- of the 21 knees, 3 revisions were required for patellar complications;
- one patellar component was loose on radiographs and there was marked patellofemoral pain in 6 knees;
- 11 / 21 knees (52%) underwent revision or were recommended for revision for patellar complications or had anterior knee pain that limited activities;
- references:
- Asymmetric patella resurfacing in total knee arthroplasty.
- Biomechanical consequences of patellar component medialization in total knee arthroplasty.
- select component size:
- component should cover cut surface;
- patella is usually wider in the medial lateral dimension than in the proximal-distal dimension;
- make certain that there is no overhang, esp. proximally & distally;
- ref: The John Insall Award: Control-matched Evaluation of Painful Patellar Crepitus After Total Knee Arthroplasty
- Depth of Patellar Resection:
- before resecting any bone, it is helpful to measure the thickness of patella, with a caliper;
- note that the average thickness of the male patella is 25 mm and that of the female 22 mm;
- it is important to exactly replace articular surface, that is resect neither to much or too little;
- amount of patella resection should equal thickness of patellar implant;
- to avoid increased patellar strains, bone patella should not be cut to a thickness of less than 12 to 15 mm;
- always know the thickness of the patellar implant before the cut is made;
- references:
- Freehand resection of the patella in total knee arthroplasty referencing the attachments of the quadriceps tendon and patellar tendon.
- The Width:thickness Ratio of the Patella. An Aid in Knee Arthroplasty
- too little resection:
- height of the patella will be increased;
- altering biomechanics of quadriceps;
- may limit flexion;
- references:
- The effect of patellar thickness changes on patellar tilt in total knee arthroplasty.
- The effect of patellar thickness on intraoperative knee flexion and patellar tracking in total knee arthroplasty
- The effect of overstuffing the patellofemoral joint on the extensor retinaculum of the knee
- Patellofemoral overstuff and its relationship to flexion after total knee arthroplasty.
- The Effect of Stuffing the Patellofemoral Compartment on the Outcome of Total Knee Arthroplasty
- Residual posterior femoral condyle osteophyte affects the flexion range after total knee replacement
- too much resection:
- worst error;
- results in a thin and mechanically weak patella that is prone to patellar fracture;
- to avoid increased patellar strains, bone patella should not be cut to thickness of less than 12 to 15 mm;
- references:
- The Effect of Patellar Thickness on Intraoperative Knee Flexion and Patellar Tracking in Total Knee Arthroplasty.
- Patellofemoral overstuff and its relationship to flexion after total knee arthroplasty.
- The effect of patellar thickness on intraoperative knee flexion and patellar tracking in total knee arthroplasty.
- Measurement of patellar thickness in relation to patellar resurfacing.
- Influence of patellar thickness on results of TKA: does a residual bony patellar thickness of <or=12 mm lead to poorer clinical outcome/complications?
- Patellar resection during total knee arthroplasty: effect on bone strain and fracture risk.
- The effect of patella preparation for total knee arthroplasty on patellar strain: a comparison of resurfacing versus inset implants.
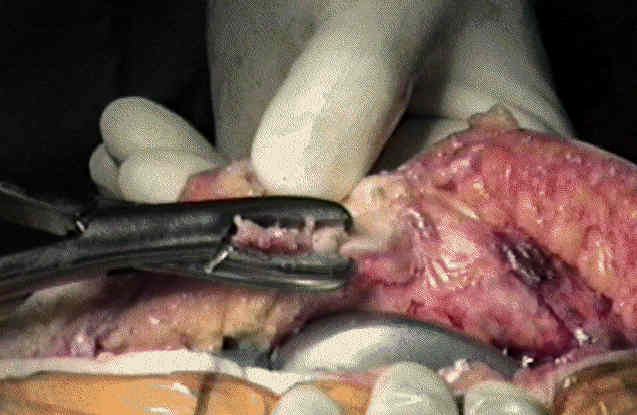
- Onset Technique of Patellar Resection:
- with this method, the articular surface of the patella is resected to flat base and the patellar implant affixed on this base;
- resect any rim osteophytes or surrounding synovial overgrowth (esp in RA pt) are removed so that the exact dimensions of bone can be ascertained;
- hazards:
- avoid inadvertent cutting of either the patellar ligament or the quadriceps tendon;
- cut should be flat and should not remove too much bone, lest fracture of the patella develop;
- avoid making asymmetrically directed cuts;
- note that medial facet is usually thicker than the lateral facet, which leads to a common error of cutting off equal amounts of bone
from both facets (ie too much bone is taken from the lateral facet) - this creates an abnormal tilt to the patella;
- proper method is to "under-resect" lateral facet, removing only subchondral bone, and continuing the cut into substance of medial facet;
- in report by Pagnano, et al, 300 consecutive primary, cemented, condylar TKAs were reviewed for presence of asymmetric patella resurfacing using a postop Merchant or sunrise patellar radiograph;
- 21 knees in 14 patients were found to have the patella asymmetrically resurfaced.
- asymmetric resurfacing typically involved inadvertent preferential resurfacing of lateral facet w/ underresection of bone from medial facet;
- all patients underwent follow-up for a minimum of 5 years, with a mean follow-up of 7.5 years;
- of the 21 knees, 3 revisions were required for patellar complications;
- one patellar component was loose on radiographs and there was marked patellofemoral pain in 6 knees;
- 11/21 knees (52%) had revision or were recommended for revision for patellar complications or had anterior knee pain that limited activities;
- ref: Asymmetric patella resurfacing in total knee arthroplasty.
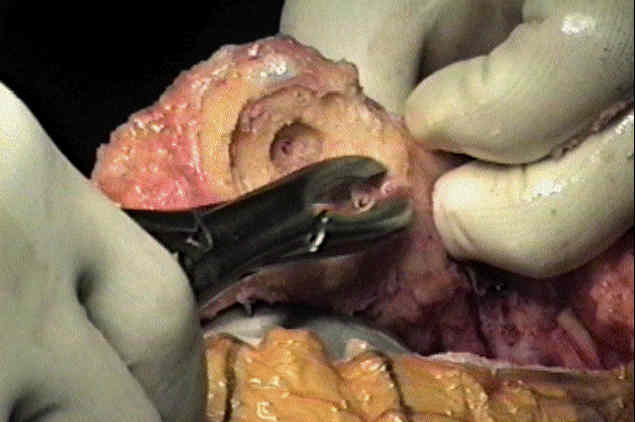
- Inset Technique of Patellar Resection:
- in this technique, the patella is held by a patella clamp, and thru clamp a channel is reamed into which patellar implant is inset;



- Access Patellar Tracking:
- with all trial components in place, the knee is taken through a series of ROMs, and the surgeon assesses for patellar subluxation and lateral tilt;
- with frank subluxation, the surgeon must reassess for component malrotation and considers lateral release
Acurate preparation of the patella during total knee arthroplasty.
Lateral Release Rates After Total Knee Arthroplasty
Patellar prosthesis positioning in total knee arthroplasty. A roentgenographic study.
Patellofemoral arthroplasty. A three- to nine-year follow-up study.
Wear and deformation of patellar components in total knee arthroplasty.
Technique for patellar resurfacing in total knee arthroplasty.
Patellofemoral function in total condylar knee arthroplasty.
Patellar Impingement against the Tibial Component after Total Knee Arthroplasty.
Anatomic dimensions of the patella measured during total knee arthroplasty.
Patellar component positioning in total knee arthroplasty.
Clinical and biomechanical assessment of patella resurfacing in total knee arthroplasty.
- Johnson and Johnson: