

- See: Medial Approach:
- Discussion:
- medial epicondyle is common origin of several flexor muscles of hand and wrist;
- when medial epicondyle is frxed, flexor muscles pull fragment distally;
- during surgical procedure care must be made to protect ulnar nerve;
- Fixation Stratedgy:
- medially directed plate fixation takes advantage of avoiding ulnar nerve, except when the distal plate screw extends over the distal-medial
portion of the condyle;
- w/ low medial column frx, a 1/3 tubular plate may be contoured around the medial condyle, which allows insertion of a interfragmentary
lag screw,
directed superiorly in the medial column (avoid the fossa);
- as mentioned, a plate placed over the distal-medial edge of the condyle will encroach on the cubital tunnel and may irritate the
ulnar nerve;
- in these patients, anterior transposition may indicated;
- implants:
- 4.0 cancellous bone screws, 3.5 mm cortex screws, or 4.5 mm canulated screws as lag screws;
- one third tubular plate may be necessary for larger fragments;
- technique:
- contour a 3.5-millimeter reconstruction plates to the medial epicondyle;
- the reconstruction plate is contoured and bent around to cradle the epicondyle;
- most distal screws are directed into medial epicondyle;
- ulnar nerve in condylar fractures:
- note that a plate or lag screw placed over the distal-medial edge of the condyle will encroach on the cubital tunnel and may
irritate the ulnar nerve;
- in these patients, anterior transposition may indicated
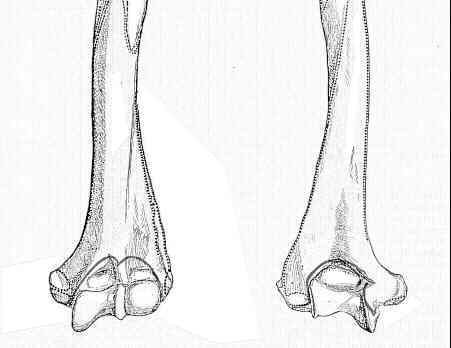
Fracture of the medial condyle of the humerus.