
- See:
- Cervical Spondylosis:
- SCIWORA Syndrome
- Discussion:
- are most frequent at C 6-7 level but also occur at C 5-6 & to a lesser extent at C4-5 & other levels;
- in relatively younger persons soft disk protrussion is more common than hard disk protrussion;
- differential diagnosis:
- types of herniation:
- intraforaminal herniation:
- most common type:
- cause predominately sensory changes;
- posterolateral type:
- occurs near near entrance zone of foramen;
- causes predominately motor changes;
- central type:
- if disc herniation occurs more to the midline (ie posterior herniation), then it compresses spinal cord in addition to, or instead
of the nerve root;
- results in cervical myelopathy:
- Symptoms:
- neck pain from nerve root compression;
- pain radiating into ipsilateral upper extremity w/ paresthesias, numbness, or weakness;
- pain & paresthesias may be intensified by neck movement, especially by extension or by lateral flexion to side of herniation, & by
coughing or straining;
- Exam:
- see: cervical radiculopathy and myelopathy
- limitation of neck extension
- downward head compression increases pt's radicular pain & paresthesias, especially if neck is flexed to side of involvment;
- shoulder abduction relief test:
- significant relief of arm pain with shoulder abduction;
- this sign is more likely to be present w/ soft disc herniation, whereas, the test is likely to be negative with radiculopathy caused by
spondylosis (osteophyte compression);
- spurling's Sign:
- mechanical stress, such as excessive vertebral motion, may exacerbate symptoms;
- the provocation of the patient's arm pain with induced narrowing of the neuroforamen
- gentle neck hyperextension with the head tilted toward the affected side will narrow the size of the neuroforamin and may exacerbate
the symptoms or produce radiculopathy;
- ipsilateral rotation of the neck will also increase radiculopathy;
- downward head compression increases the patient's radicular pain and paresthesias, especially if the neck is flexed to the side of
involvment;
- provocation of pt's arm pain w/ induced narrowing of neuroforamen
- oblique cervical extension augments root compression & increases symptoms;
- lower motor neuron dysf(x) (muscle weakness & hypotonia, reduction of deep tendon reflexes) at level of cord compression;
- upper motor neuron dysfunction (spasticity, clonus, increased deep tendon reflexes, Babinski's sign, reduction of sensation) below level;
- loss of erection, bladder, & bowel f(x) may occur;
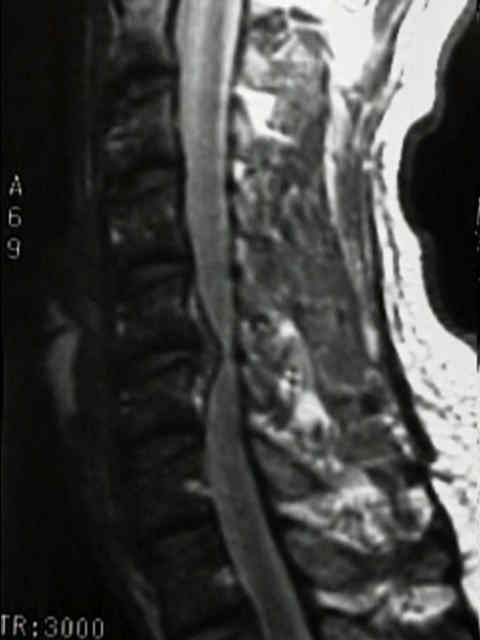
- MRI: 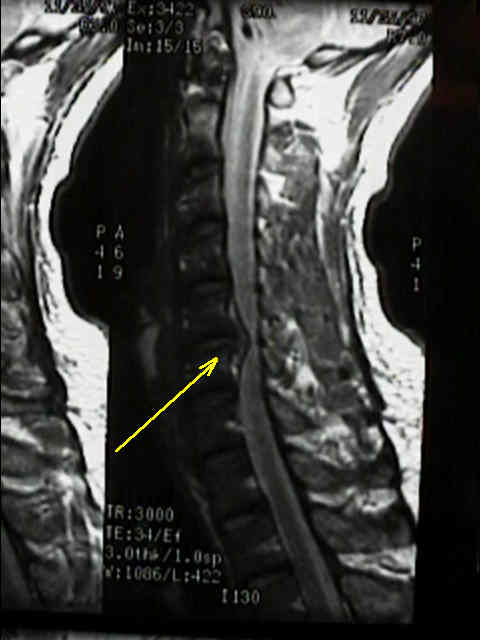
- Treatment:
- surgery is usually performed by a posterior approach thru a hemi-laminectomy or by an anterior approach to approach the intervebral disc;
- anterior approach:
- anterior approach tends to be more popular with orthopaedic surgeons and is especially indicated for central or peri-central
disc herniation;
- decompression is usually followed by arthrodesis;
- posterior approach:
- posterior decompression is a smaller operation that takes less time and does not require a bone graft;
- posterior decompression is most indicated for far-lateral disc herniation
Surgical management of cervical soft disc herniation. A comparison between the anterior and posterior approach.
Original Text by Clifford R. Wheeless, III, MD.
Last updated by Data Trace Staff on Wednesday, December 21, 2011 4:26 pm