

- See:
- scaphoid fracture:
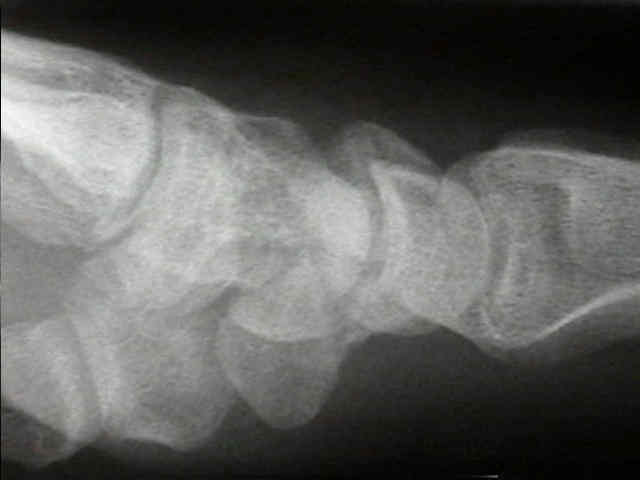
- non diagnositic x-ray
- bone scan for scaphoid frx:
- CT scan evaluation
- radiology of hand & wrist:
- radiology scapholunate dislocation
- Discussion:
- classification: complete fractures tend to fall into distinct categories;
- about 1/9 scaphoid fractures will be incomplete;
- complete fractures tend to fall into distinct categories;
- tubercle frx
- these fractures may often be mistaken for dorsal sulcus frx, since collapse at the frx sitereduces its length on the PA film,
which falsely makes it appear more distal;
- transverse waist frx
- proximal pole frx
- dorsal sulcus frx (oblique in the plane of the dorsal sulcus):
- these frx occur in the line of the dorsal sulcus (which is 45 deg to the surgical waist);
- frx line starts at the dorsal apex of the ridge adjacent to the lunate and runs obliquely;
- these fractures may often be mistaken for dorsal sulcus frx, since collapse at the frx site
reduces its length on the PA film, which falsely makes it appear more distal;
- this type of frx pattern is unstable and often leads to the humpback deformity;
- any displacement that is shown at frx site indicates significant instability, making internal fixation rx of choice;
- note that increased fracture obliquity is associated w/ increase scaphoid instability;
- on both PA and lateral views note whether there is any carpal instability, which might represent trans-scaphoid perilunate dislocation;
- Radiographic Views:
- semi-pronated oblique PA view:
- best view for assessing dorsal sulcus fractures, and can also help evaluate waist frx displacement;
- semi-supinated oblique AP view:
- AP w/ 45 deg supination & ulnar deviation (ulnar deviation rotates the scaphoid into a horizontal position and puts scaphoid in
profile;
- best view to assess proximal pole fractures, and is also the best for assessing the humpback deformity;
- PA of wrist in ulnar deviation:
- most useful for proximal pole frx;
- ulnar deviation diminishes extent to which surrounding carpals overlap image of scaphoid;
- the PA view may not optimally show a waist frx because the scaphoid tubercle overlaps the waist (due to the flexion posture of the
scaphoid);

- ulnar deviated PA w/ 20 deg tube angulation toward elbow
- this view takes into consideration the flexion posture of the scaphoid, so that the tubercle no longer overlaps
the waist;
- this view is most specific for scaphoid waist fractures;
- intercarpal angulation (PA view):
- normal angle is 30 deg (plus or minus 5 deg);
- angle formed by two lines formed by each pole of the scaphoid (lines are formed by the perpendicular
lines drawn from the articular surfaces of the proximal and distal scaphoid articulations)
- the distal scaphoid line is formed by the line drawn perpendicular to the STT joint;
- the proximal scaphoid line is formed by the line drawn perpendicular to the line drawn that bisects the proximal pole between
the capitate and radius articular surfaces;
- lateral view:
- ensure that a true lateral radiograph is taken (w/ wrist in neutral position);
- normally the scaphoid is flexed 47 deg w/ respect to the co-linear radius-lunate-capitate articulations;
- there is concern w/ capitolunate angle > 10 deg, & almost certain problem when angle is > 20;
- on both PA and lateral views note whether there is any carpal instability, which might represent a trans-scaphoid perilunate dislocation;
- w/ significant scaphoid humpback deformity, a DISI deformity may be created;
- lateral scaphoid angulation:
- normal angulation is 25 deg (plus or minus 5 deg);
- proximal scaphoid line:
- may be drawn from the perpendicular of the distal radius articular surface or can be judged from the position of the lunate;
- distal scaphoid line is drawn perpendicular to the STT joint articular surface;
- CT Scan Evaluation of Scaphoid Frx

- Case Examples:

 ***
*** 

The anatomy of acute scaphoid fractures: a three-dimensional analysis of patterns.
