

- See: Notchplasty:
- Technique:
- preparation - tibial tunnel:
- tibial tunnel is created prior to femoral tunnel;
- a more medial to lateral tunnel placement, will cause the a more medial to lateral femoral tunnel;
- femoral tunnel must be oriented in a somewhat lateral direction, in order to have the guide wire to exit distal to tourniquet;
- preparation - femoral tunnel:
- knee joint is flexed to at least 90 deg, which opens up the notch;
- in saggital plane, guide wire should pierce roof of the inter-condylar notch at a point about 6 mm anterior to posterior edge;
- 6 mm offset guide is useful to achieve a precise measurement;
- in axial plane, the guide wire should pierce notch at 1 to 2 O'clock position (left knee) or the 10-11 O'clock position (right knee);
- if tibial tunnel does not allow easy access to posterior aspect of intercondylar notch, additional knee flexion will move guide wire posteriorly;
- references:
- Femoral aimer deformation: Potential cause for altered femoral tunnel placement in anterior cruciate ligament surgery.
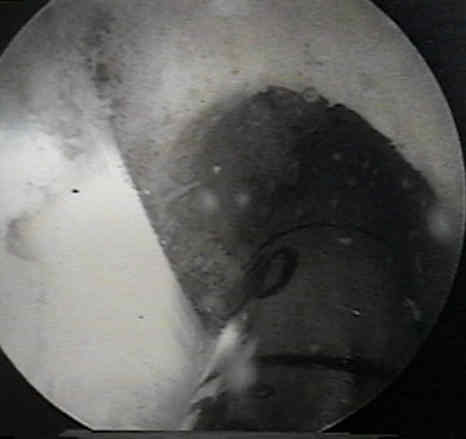
- reaming:
- a cannulated dill (10 mm) is placed over the guide wire and is reamed initially to a depth of 4-5 mm;
- drill is backed out, and the foot print is examined for possible "blow out" of the back wall
- note that geometry of posterior cortex is in MD's favor, hence if there is doubt about the back wall, surgeon can ream several
millimeters further and then reassess the situation;
- cannulated reamer is then reamed to a depth of about 30 to 35 mm:



- as these radiographs demonstrate, it is difficult to place the femoral tunnel at the 2 o'clock (or 10 o'clock) position which is necessary to
properly restore the anatomy
Femoral aimer deformation: Potential cause for altered femoral tunnel placement in anterior cruciate ligament surgery.
- Technique:
- preparation - tibial tunnel:
- tibial tunnel is created prior to femoral tunnel;
- a more medial to lateral tunnel placement, will cause the a more medial to lateral femoral tunnel;
- femoral tunnel must be oriented in a somewhat lateral direction, in order to have the guide wire to exit distal to tourniquet;
- preparation - femoral tunnel:
- knee joint is flexed to at least 90 deg, which opens up the notch;
- in saggital plane, guide wire should pierce roof of the inter-condylar notch at a point about 6 mm anterior to posterior edge;
- 6 mm offset guide is useful to achieve a precise measurement;
- in axial plane, the guide wire should pierce notch at 1 to 2 O'clock position (left knee) or the 10-11 O'clock position (right knee);
- if tibial tunnel does not allow easy access to posterior aspect of intercondylar notch, additional knee flexion will move guide wire posteriorly;
- references:
- Femoral aimer deformation: Potential cause for altered femoral tunnel placement in anterior cruciate ligament surgery.
- reaming:
- a cannulated dill (10 mm) is placed over the guide wire and is reamed initially to a depth of 4-5 mm;
- drill is backed out, and the foot print is examined for possible "blow out" of the back wall
- note that geometry of posterior cortex is in MD's favor, hence if there is doubt about the back wall, surgeon can ream several
millimeters further and then reassess the situation;
- cannulated reamer is then reamed to a depth of about 30 to 35 mm:






- as these radiographs demonstrate, it is difficult to place the femoral tunnel at the 2 o'clock (or 10 o'clock) position which is necessary to
properly restore the anatomy
Femoral aimer deformation: Potential cause for altered femoral tunnel placement in anterior cruciate ligament surgery.
Ensuring accurate femoral guide pin placement in anterior cruciate ligament reconstruction.
Original Text by Clifford R. Wheeless, III, MD.
Last updated by Clifford R. Wheeless, III, MD on Tuesday, March 19, 2013 6:23 pm