
- Resection of the Distal Femur:
- cushing rongeur is used to remove osteophytes in medial & lateral aspects of the femoral condyles as well as the intercondylar space;
- this avoids, possible mis-sizing of the femoral component;
- femoral IM alignment rod: (discussion)
- mechanical axis
- anatomic axis
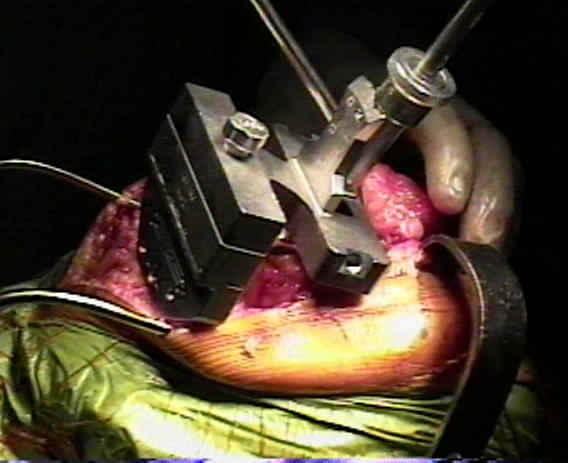
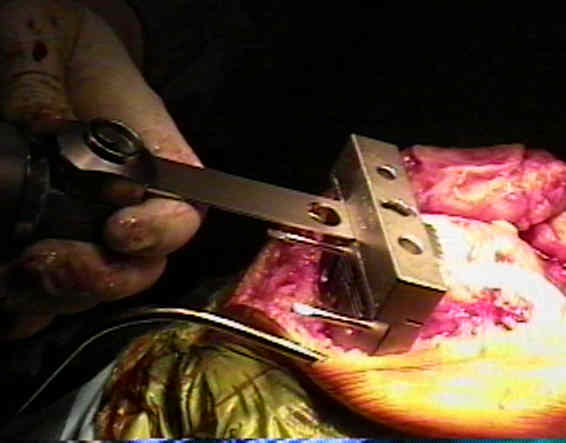
- distal femoral cutting guide:
- depth of cut:
- generally this is set for a length which makes up for the length of the femoral component (usually 8-9 mm);
- often surgeons will add, 1-2 mm to this length;
- if the patient has a knee flexion contracture, then consider cutting upto 2-3 mm beyond the templated length of the
femoral component;
- note, however, that it is important to avoid elevation of joint line, in which case the surgeon should select
a posterior stabilized knee rather than a PCL retaining component:
- author's preferred technique:
- note that the extension space will be affected by the ACL, deep MCL, and posteromedial capsule;
- 1/2 inch osteotome is used to elevate deep MCL and posteromedial capsule, and rongeur is used to remove ACL;
- once these releases have been completed, then reassess the delta change of knee extension (compared to preop);
- this technique will demonstrate that many patients that would have "required" elevation of the joint line (because
of preop contracture), will not require excessive resection of the distal femur;
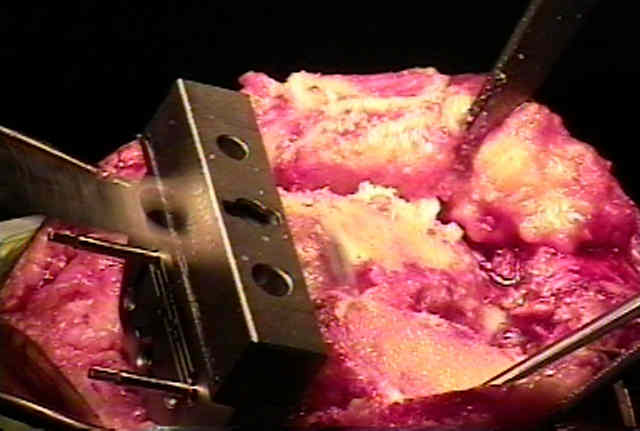
- pitfalls of cutting jig:
- note that some patients may have a prominent medial trochlear ridge which will have the effect of "artificially"
elevating the distal femoral cutting guide off of the end of the femur;
- this will be manifest by an abnormally large gap over the lateral femoral condyle;
- the result will be an inadequate distal femoral cut and reduced extension gap;
- angulation of cut:
- ideally the tibio-femoral articulation should have an angulation of 3 to 7 deg;
- in early TKR designs, proximal tibia was cut in upto 3 deg of varus, which meant that the distal femoral cut was made in
7- 9 deg of valgus;
- if the proximal tibial cut is to be cut in neutral (this is now standard), then femoral cutting guide is set for the appropriate
right or left valgus angulation of +5 to 7 deg (in the tall thin patient try +5 deg, & in short obese patient try 7 deg);
- if the alignment rod is found to be too medial, then consider changing the valgus alginment from 5 deg to 6-7 deg;
- references:
- Natural distribution of the femoral mechanical-anatomical angle in an osteoarthritic population and its relevance to total knee arthroplasty.
- 5 degrees to 6 degrees of distal femoral cut for uncomplicated primary total knee arthroplasty: is it safe?
- Errors in Knee Alignment Using Fixed Femoral Resection Angles


The Variability of Intramedullary Alignment of the Femoral Component During Total Knee Arthroplasty.
Coronal alignment in total knee arthroplasty: just how important is it?
An in vivo study of the effect of distal femoral resection on passive knee extension.