
- See:
- Sliding Screw Insertion Technique
- Sliding Hip Screw w/ Unstable Intertroch Frx
- Subtrochanteric Fractures
- Discussion:
- sliding screw plate devices have proved to be more successful for subtroch frx than earlier implants for proimal femur;
- sliding permits sl medial displacement of shaft in relationship to head & neck fragments;
- this tends to reduce the beding moment and resulting forces that lead to collapse of medial butress and varus displacement;
- for sliding to occur, plate must not be fixed w/ screws into proximal frag;
- therefore, implant is most useful in most proximal of subtroch frx;
- classifaction and frx stability:
- internal fixation for proximal femur frx counteracts deforming forces;
- successful treatment restores medial cortex by secondary bone healing w/ callus, by exact reduction of frx fragments followed by secure healing, or by medial bone grafting w/ subsequent consolidation;
- when the medial cortex is reconstituted, a lateral plate acts as tension band and is subjected to a bending load;
- distal subtrochanteric frx:
- for sliding hip screw to function optimally, sliding component must cross fracture site;
- more distal frx are treated w/ either an IM Nail or a 95 deg fixed blade plate;
- the latter device improves the fixation of the proximal fragment & acts as lateral tension band if the medial cortex is intact;
- lower fractures tend to do better w/ AO slide pate fixation if medial cortex can be reconstituted;
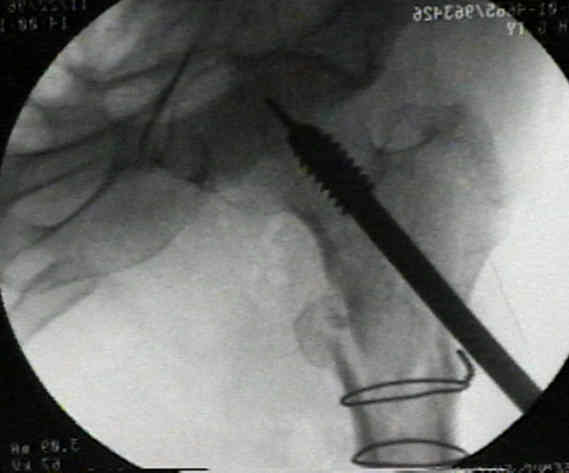
- the following example is self explanatory as to why sliding screws should be used w/ caution in treating subtrochanteric fractures;



- valgus reduction:
- readily achieved with the compression screw;
- minimizes the bending moment applied to proximal femur and implant & reduces risk of varus collapse & fixation failure;
- valgus reduction and medial shaft displacement may permit lateral cortex to accept some of compressive load normally borne by medial side of the proximal femur;
- plate angle:
- for sliding component to cross the frx site in subtrochanteric fractures, a high plate angle w/ long side plate must generally be used;
- as w/ intertroch frx, the sliding screw should allow lateral settling of the head and neck onto the shaft fragment (in effect medializing the shaft fragment);
- w/ use of high plate angles, medialization of the femoral shaft will often occur which further reduces moment arm length across the frx site;
- guide pin placement:
- guide pin is placed parallel to the calcar, just medial and inferior to the axis of the femoral neck;
- w/ use of a high plate angle, it is important to avoid positioning the guide pin superior to the center of the femoral neck in order to avoid postoperative penetration of lag screw into the acetabulum;
- inserting the screw inferior to the center of the femoral head will have the beneficial effect of allowing medialization of the distal fragment, loading sharing of the proximal and distal bone fragments, and a decrease in the moment arm across the frx site;
- inclusion of comminuted fragments;
- avoid creating a defect in the medial cortex of the proximal femur;
- w/o excessive stripping soft tissue from bone, large comminuted frags may be anatomically reduced to reconstruct medial cortex;
- if frx comminution is not ammenable to internal fixation, it is essential to insert the lag screw low in the femoral neck and head and to use a high plate to effect a medialization of the femoral shaft fragment;
- w/ shaft medialization, comminution of the greater trochanteric and lesser trochanteric fragments should occur and should incorporate into the frx callus;
- any significant medial defect or zone where healing may be delayed should be augmented with a graft of corticocancellous bone;
- generally at least 6 cortical screws w/ firm bicortical purchase need to be inserted below the lowest level of comminution;
case examples:





Treatment of subtrochanteric femur fractures using the dynamic condylar screw.