Tom Large, MD
Ben Kam, MD
C. Demonstrate knowledge of the indications for and ability to implement emergent orthopedic interventions (tourniquet, etc.)
I. Tourniquets
A. Prehospital tourniquet use shown to have significant beneficial effect on blood loss, shock, and mortality without increased risk for amputation or conversion to higher amputation levels1, 2
B. Application of tourniquets taught as part of echelon I (self-aid, buddy care) course to all military personnel
C. Combat Application Tourniquet System (CATS) tourniquet (
see figure 12, figure 13) is most frequently used military field tourniquet and is supplied in individual first aid kits (IFAKs)
D. Tourniquets should be applied to upper thigh or upper arm for extremity injuries
E. Tourniquets best removed in operating room and may be replaced with standard pneumatic tourniquets
F. Coordination of tourniquet removal with resuscitating anesthesiologist or traumatologist is imperative, as systemic response to blood redistributing in limb and reperfusion of blood-starved tissues releasing cellular damage by-products is expected
II. Fractures/Dislocations (
see figure 14, figure 15)
A. Dislocated joints should be reduced and held with external fixation or percutaneous wires and pins as necessary
B. Acute management of fractures generally involves same principles and methods used in civilian fracture setting. External fixation for many open fractures, anticipating delayed definitive reconstruction in mass casualty situations
C. Fracture reductions should restore length and alignment and be held with external fixators, percutaneous pins, wires, or a splint for closed, lower energy injury, as would be indicated in civilian sector (i.e., distal radius fractures, metacarpal or metatarsal fractures, etc.)
D. External fixation allows for stabilization of soft tissue injury, protection of any associated vascular repair or reconstruction, and easy transport of patient with better pain control from improved fracture stabilization
III. Internal Fixation
A. Definitive internal fixation may need to be delayed and may depend on equipment, facility, and evacuation factors
1. generally contraindicated in military/austere environment due to increased risk of infection
2. may be contraindicated in disaster setting, depending on availability of adequate equipment and facilities
B. Reductions should be held with external fixation devices and percutaneous k-wires
C. Generally, only fracture or dislocation that should be considered for open reduction and internal fixation in military theater is femoral neck fracture in young patient
1. highly controversial
2. if anatomic reduction can be achieved via closed means, fracture can be held with combination of long Steinmann pins and/or long external fixation pins incorporated into femur-based construct; may be combined with percutaneous capsulotomy
3. if anatomic reduction cannot be achieved and held via closed means, consideration for open reduction and internal fixation can be entertained, preferably at facility with adequate equipment and sterility
4. limited available data support safe and judicious use of internal fixation in military theater8-10
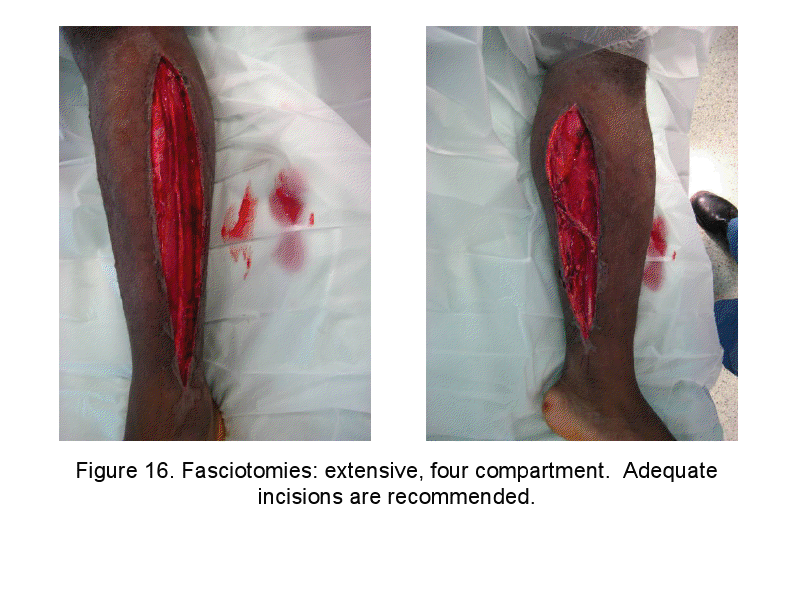
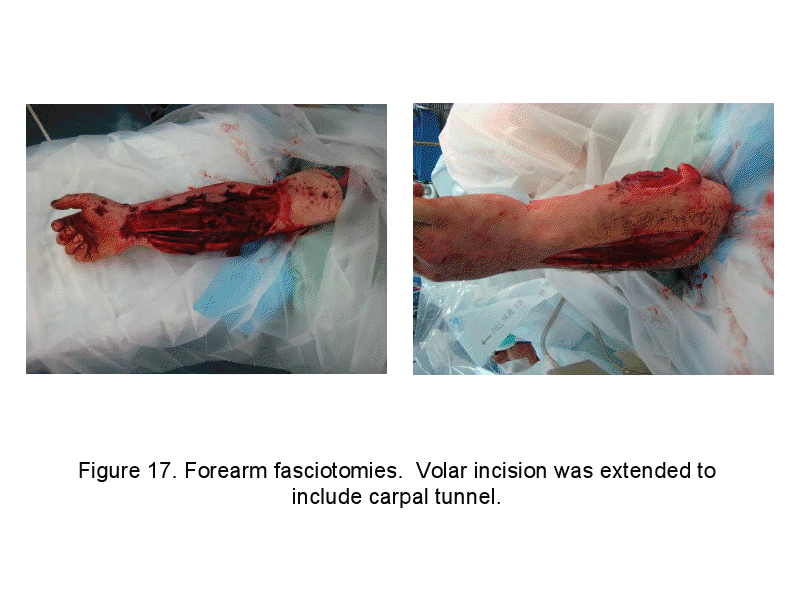
A. Compartment syndrome is major consideration with crushing/blast/high energy injuries to lower extremity
B. Key to management is early clinical diagnosis and early intervention to include prophylactic treatment with fasciotomy
C. May be limited ability to measure compartment pressures in combat/disaster zone; fasciotomy advocated when clinical concern exists
D. Most commonly cited clinical signs for diagnosis
1. pain out of proportion
2. pain with passive stretch
3. palpably tense compartments
E. Most commonly, compartment syndrome occurs in anterior and deep posterior compartments of leg
1. some 45% caused by tibia fracture4
2. incidence of compartment syndrome higher in open fractures than closed
F. Fasciotomy not recommended in established diagnosis of compartment syndrome, with warm ischemia time greater than 12 hours
G. Fasciotomy may not be indicated in conjunction with escharotomy in burn patients in absence of etiologies for compartment syndrome (crush, fracture, polytrauma, overresuscitation, or electrical injury)
References
1. Emergency War Surgery, 3rd ed. Borden Institute, Walter Reed Army Medical Center. 2004, ch. 22, pp 22.9-22.14.
2. Kragh JE Jr, O’Neill ML, Walters TJ et al. Minor morbidity with emergency tourniquet use to stop bleeding in severe limb trauma: research, history, and reconciling advocates and abolitionists. Mil Med. 2011;176:817-23.
3. Emergency War Surgery, 3rd. ed. Borden Institute, Walter Reed Army Medical Center. 2004, ch 26, pp 26.1-26.8.
4. Kragh J. Joint Theater Trauma System Clinical Practice Guidelines: Compartment Syndrome and the Role of Fasciotomy in Extremity War Wounds. Joint Theater Trauma Services, draft Jan. 2009.
5. Nessen S, Lounsbury DE, Hetz SP. War surgery in Afghanistan and Iraq. Dept. of the Army: Borden Institute, 2008.
6. Noordin S, McEwen JA, Kraugh JF Jr., et al. Surgical tourniquets in orthopaedics. J Bone Joint Surg Am. 2009;91(12):2958-2967.
7. Pollak AN, Calhoun JH. Extremity war injuries: state of the art and future directions. J Am Acad Orthop Surg. 2006;14(10):S1-S213.
8. Stinner DJ, Keeney JA, Hsu JR, et al. Outcomes of internal fixation in a combat environment. J Surg Orthop Adv. 2010;19:49-52.
9. Keeney JA, Ingari JV, Mentzer KD, Powell ET. Closed intermedullary nailing of femoral shaft fractures in an echelon III facility. Milit Med. 2009;174:124-128.
10. Mody RM, Zapor M, Martzell JD, et al. Infectious complications of damage control orthopedics in war trauma. J Trauma. 2009;67(4):758-761.
The view(s) expressed herein are those of the author(s) and do not reflect the official policy or position of Brooke Army Medical Center, the U.S. Army Medical Department, the U.S. Army Office of the Surgeon General, the Department of the Army, Department of Defense or the U.S. Government.
Materials and support for The Disaster Preparedness Toolbox is provided by Lt Col. Ky Kobayashi, MD and Col. Benjamin Kam, MD.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}