
CPT Brendan Masini, MD
A. Define compartment syndrome and describe the diagnostic limitations presented by an austere environment
I. Acute Compartment Syndrome
A. Occurs when pressure within myofascial compartment exceeds threshold perfusion gradient across capillary beds
1. if unchecked, leads to tissue hypoxia and cell death
2. ischemia and necrosis of muscles can occur even if arterial pressure remains high enough to preserve pulses
B. Conditions that can lead to compartment syndrome
1. fractures, burns, gunshot wounds, other high-energy mechanisms of injury, including blast trauma
2. common in austere combat and disaster environments
C. Austere medical environment highly variable in terms of available diagnostic equipment and surgical assets
1. especially germane to discussion of compartment syndrome, which has historically been a clinical diagnosis
2. frequently augmented with compartment pressure measurements
D. Important for surgeons to understand how to make diagnosis of compartment syndrome and provide treatment in austere environment with limited resources
II. Clinical Picture
A. Acute compartment syndrome may occur following any extremity trauma
B. Clinician should have high index of suspicion
C. Clinical scenarios
1. open fractures
2. closed fractures
3. penetrating wounds
4. crush injuries
5. vascular injuries
6. reperfusion following vascular repairs
D. Important to realize that fascial defect caused by injury is often insufficient for decompression of associated compartment
III. Diagnosis
A. Classic physical exam findings
1. pain
2. pallor
3. pulselessness
4. paresthesias
5. paralysis
B. Pain with passive stretch is most sensitive clinical finding prior to onset of ischemic dysfunction
C. Palpation of tense or swollen compartments may add some data in clinical decision making process, however recent data points to inconsistency of this form of diagnosis1
D. In obtunded or unresponsive patient, compartment pressure measurements may be only objective criteria for diagnosis
E. Austere environment recommendation
1. in absence of invasive monitoring, proceed with best clinical information available
2. early clinical diagnosis
a. pain out of proportion
b. pain with passive stretch
c. tense, swollen compartment
IV. Invasive Measurements
A. In austere environment, equipment for invasive compartment pressure measurement may not be available
1. serial examination may not be feasible in patients rapidly being prepared for evacuation to higher echelons of care
2. understanding of multiple compartment measuring modalities allows surgeon ability to utilize common equipment on hand
B. Measurement method
1. Whiteside’s technique (infusion) (see figure 1)
.jpg){kind=link}
a. equipment – use either
i. manometer or arterial line pressure monitor with transducers, IV tubing, 18-gauge needles, 3-way stopcock, syringe of normal saline
ii. electronic monitor (Stryker STIC, Howmedica slit catheter)
b. needle selection for measurement of compartments does matter
i. side-ported needle or slit catheter are both equally effective and accurate
ii. standard simple needle consistently overestimates pressures by average of 19 and 18 mmHg, compared with slit catheters and side-ported needles, respectively2
c. location of measurement
i. high variability found with measurements within single compartments
ii. pressure most reproducibly elevated within 5 cm of tibia fracture
iii. may extrapolate to other body regions3
d. in contrast, proximal vascular injury, leading to ischemia perfusion injury, will likely cause more uniform elevation in pressure throughout a compartment
2. austere environment recommendation
a. measurement of compartment pressures not necessary if clinical suspicion exists and equipment limited
b. consider prophylactic fasciotomy in patients with high energy wounds, vascular repair, or high index or suspicion
c. special consideration should be given to patients who are intubated, comatose or sedated, have closed head injuries, circumferential dressings or casts, or are facing prolonged transport
References
1. Shuler FD, Dietz MJ. Physician’s ability to manually detect isolated elevations in leg intracompartmental pressure. J Bone Joint Surg. 2010;92:361-367.
2. Moed BR, Thorderson PK. A comparison of the slit catheter, side-ported needle, and simple needle. J Bone Joint Surg Am. 1993;75(2):231-235.
3. Heckman MM, Whitesides TE Jr, Grewe SR, et al. Compartment pressure in association with closed tibial fractures: the relationship between tissue pressure, compartment, and the distance from the site of the fracture. J Bone Joint Surg Am. 1994;76:1285-1292.
B. Demonstrate proper fasciotomy techniques for the upper and lower extremities
I. Onset of Tissue Injury
A. Muscle and nerves may survive up to 4 hours of ischemia without development of irreversible damage
B. Nerves may have neuropraxic damage at 4 hours, however greater ischemic time will produce irreversible injury including axonotmesis at 8 hours
II. Indications for Fasciotomy in Austere Combat Environment (Emergency War Surgery)
A. 4-6 hour delay after vessel injury
B. Combined vein and artery injury
C. Arterial ligation
D. Concomitant fracture/crush, severe soft-tissue injury, muscle edema or patchy necrosis
E. Tense compartment/compartment pressures exceeding 40 mmHg
F. Prophylactic for patients with prolonged transport times or long periods without observation (no surgical care available en route)
III. Upper Extremity Fasciotomy
A. Brachium
1. arm has two compartments
a. anterior (biceps, brachialis)
b. posterior (triceps)
2. fasciotomy technique
a. lateral skin incision from deltoid insertion to lateral epicondyle
b. spare larger cutaneous nerves
c. at fascial level, intermuscular septum between anterior and posterior compartment is identified and fascia overlying each compartment is released with longitudinal incisions; protect radial nerve as it passes through intermuscular septum from posterior compartment to anterior compartment just below fascia (see figure 2)
.png){kind=link}
B. Antebrachium
1. forearm has three compartments
a. mobile wad proximally
b. volar compartment
c. dorsal compartment
2. fasciotomy technique – will consist of longitudinal centrally placed incision over extensor compartment and curvilinear incision on flexor aspect beginning at antecubital fossa (see figure 3 and figure 4)
{kind=link}
.png){kind=link}
a. palmar incision is made between thenar and hypothenar musculature in palm, releasing carpal tunnel as needed
b. incision is extended transversely across wrist flexion crease to ulnar side of wrist, then arched across volar forearm, back to ulnar side at elbow (see figure 5 and figure 6)
{kind=link}
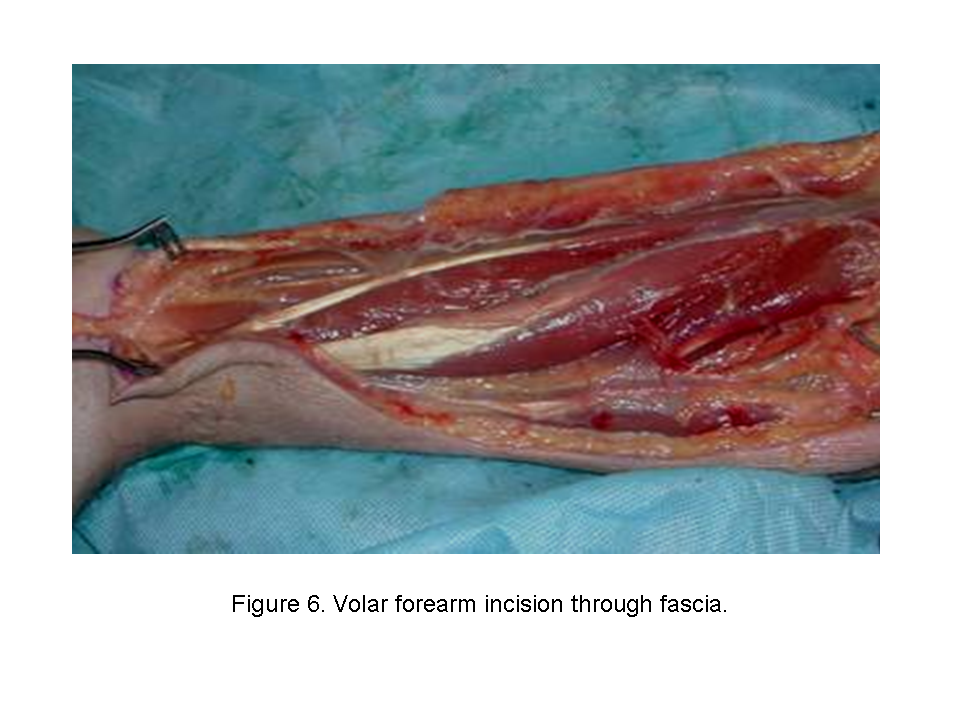{kind=link}
c. at elbow, just radial to medial epicondyle, incision is curved across elbow flexion crease; deep fascia is then released
d. at antecubital fossa, fibrous band of lacertus fibrous overlying brachial artery and median nerve is carefully released
e. this incision allows for soft tissue coverage of neurovascular structures at wrist and elbows and prevents soft tissue contractures from developing at flexion creases
f. second straight dorsal incision can be made to release dorsal compartment, reaching proximally to release mobile wad if necessary
3. complications
a. Volkmann’s ischemic contracture may develop in delayed diagnosis of forearm compartment syndrome
b. may result in ischemic contracture with severe muscle fibrosis and neuropathy and functionless extremity with few treatment options
C. Hands
1. hand has 10 separate fascial compartments
a. 4 dorsal interossei
b. 3 volar interossei
c. thenar muscles
d. hypothenar muscles
e. adductor pollicis
2. fasciotomy technique – consists of 4 incisions (see figure 7)
{kind=link}
a. one incision on radial side of thumb metacarpal releases thenar compartment (figure 8)
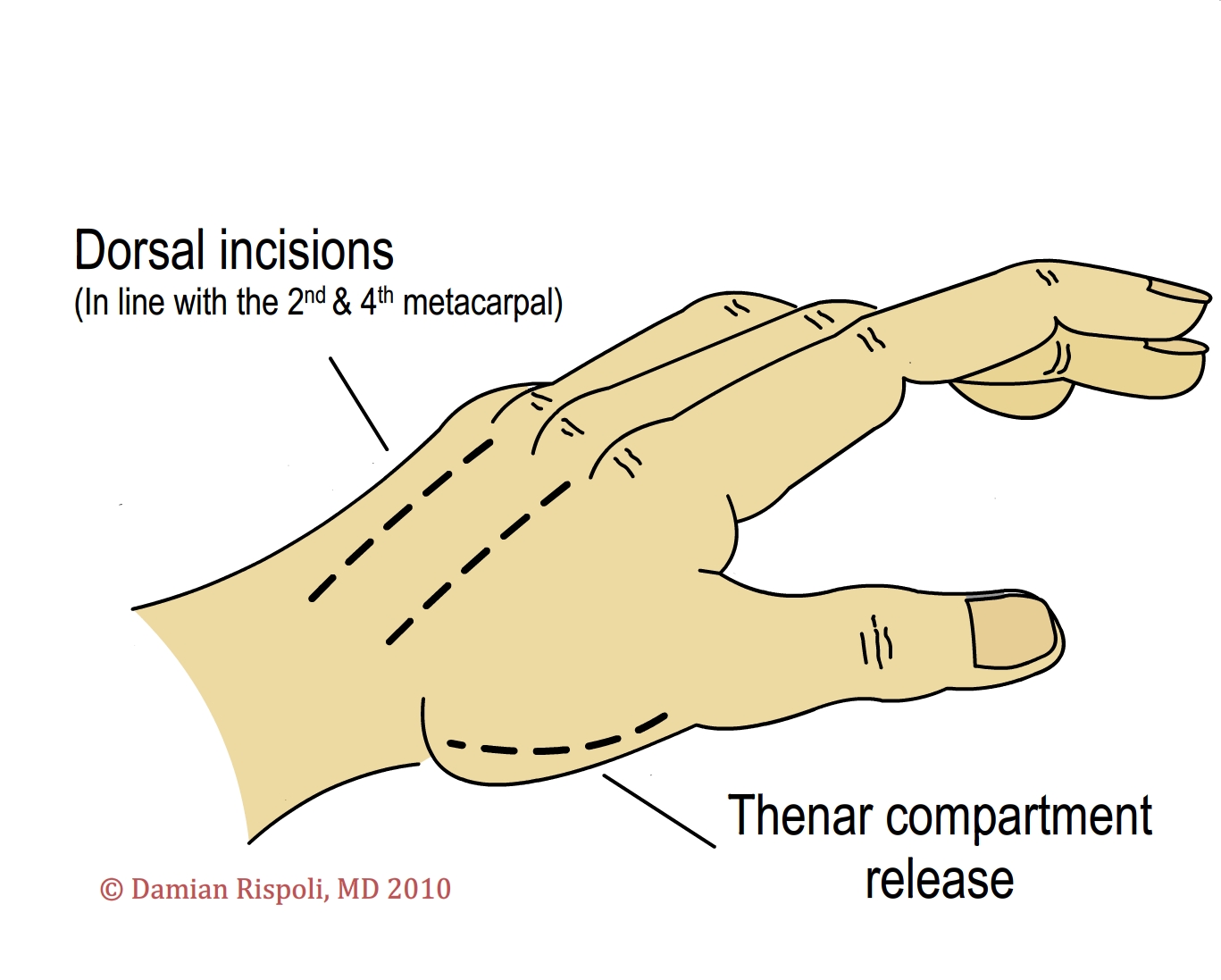{kind=link}
b. dorsal incision over index finger metacarpal used to release first and second dorsal interossei and to reach ulnar-to-index finger metacarpal and to release volar interossei and adductor pollicis
c. dorsal incision over ring finger metacarpal used to release third and fourth dorsal interossei and to reach down along radial aspect of ring finger and small finger metatarsal to release volar interossei
d. incision placed at ulnar aspect of small finger to release hypothenar muscles
e. although compartments not well defined in fingers, grossly edematous fingers may require release of dermal and fascial constriction; care should be taken to place skin incision away from neurovascular bundles
IV. Lower Extremity Fasciotomy
A. Thigh
1. thigh has three compartments
a. anterior (quadriceps)
b. medial (adductors)
c. posterior (hamstrings)
2. acute compartment syndrome uncommon in thigh because of large potential volume of compartment as well as blending of fascial compartments of thigh with hip, potentially allowing extravasation of blood outside compartment
3. risk factors for acute compartment syndrome of thigh
a. systemic hypotension
b. history of external compression of thigh
c. use of military antishock trousers
d. coagulopathy
e. vascular injury
f. severe blunt trauma to thigh
g. over-lengthening with skeletal traction (reduces volume of compartments)
4. fasciotomy technique (see figure 9)
{kind=link}
a. lateral incision made from greater trochanter to lateral condyle of femur
b. iliotibial band incised and vastus lateralis reflected off intermuscular septum bluntly, releasing anterior compartment (see figure 10)
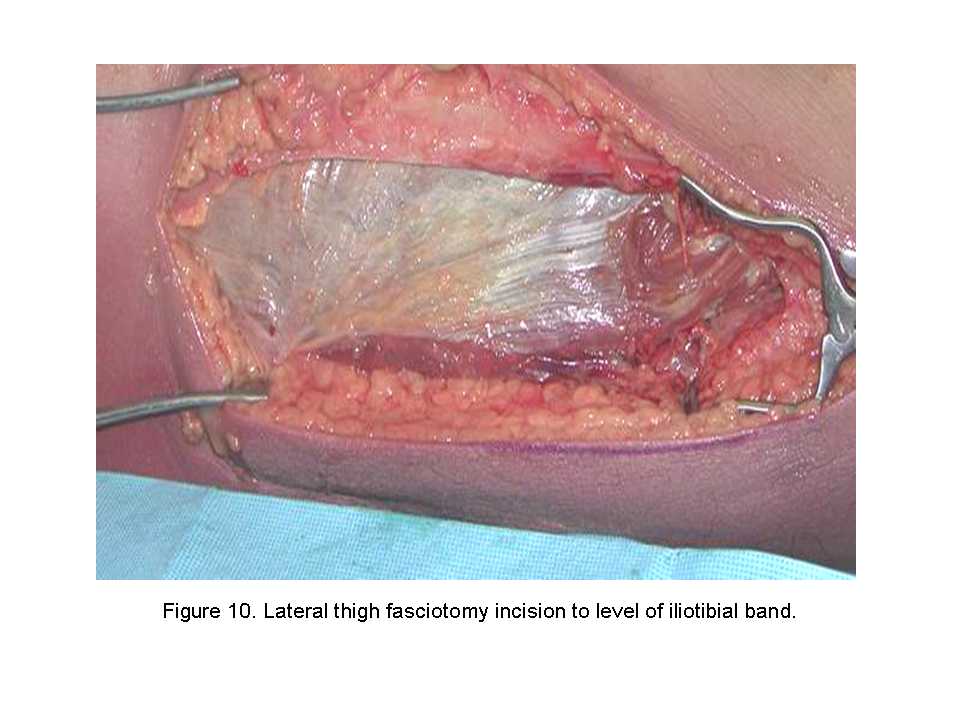{kind=link}
c. intermuscular septum then incised the length of the incision, releasing posterior compartment (this release of intermuscular septum should not be made close to femur because there are a series of perforating arteries passing through septum from posterior to anterior near bone) (see figure 11)
.png){kind=link}
d. medial adductor compartment released through separate anteromedial incision (see figure 12)
{kind=link}
B. Leg
1. leg has four compartments
a. lateral (peroneal brevis and longus)
b. anterior (extensor hallucis longus, extensor digitorum longus, tibialis anterior, and peroneus tertius)
c. superficial posterior (gastrocnemius and soleus)
d. deep posterior (flexor hallucis longus, flexor digitorum longus, and tibialis posterior)
d. deep posterior (flexor hallucis longus, flexor digitorum longus, and tibialis posterior)
2. deep posterior compartment is most commonly affected followed by the anterior compartment
3. fasciotomy technique (see figure 13)
{kind=link}
a. incisions must extend entire length of calf to release all of compressing fascia and skin
b. lateral incision made centered between fibula and anterior tibial crest (see figure 14)
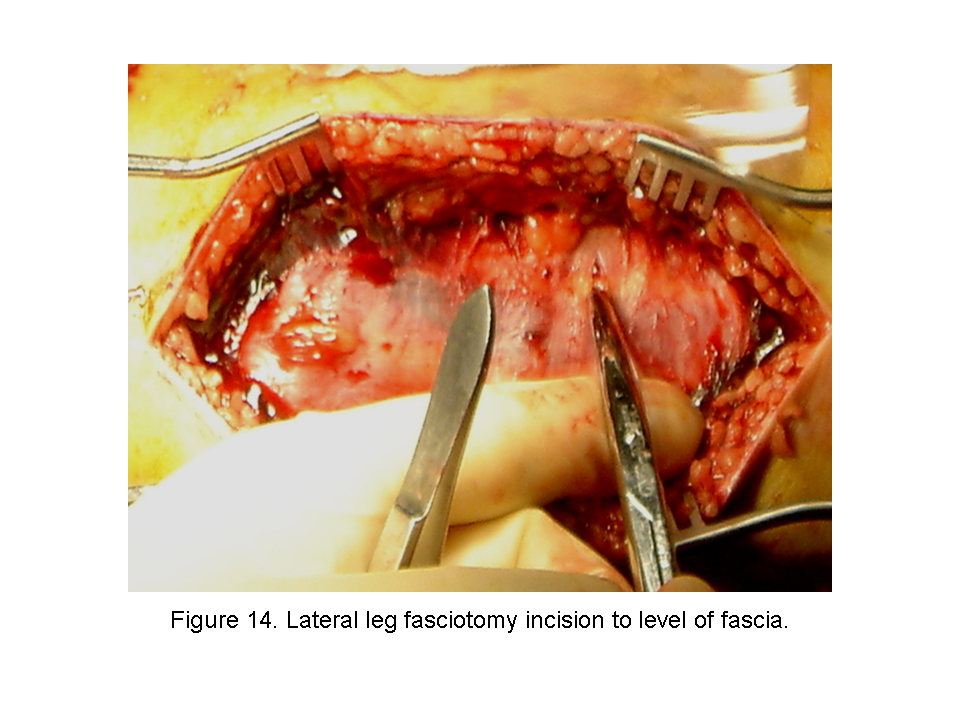{kind=link}
c. lateral intermuscular septum and superficial peroneal nerve are identified and anterior compartment is released in line with tibialis anterior muscle, proximally toward tibial tubercle and distally toward anterior ankle (see figure 15)
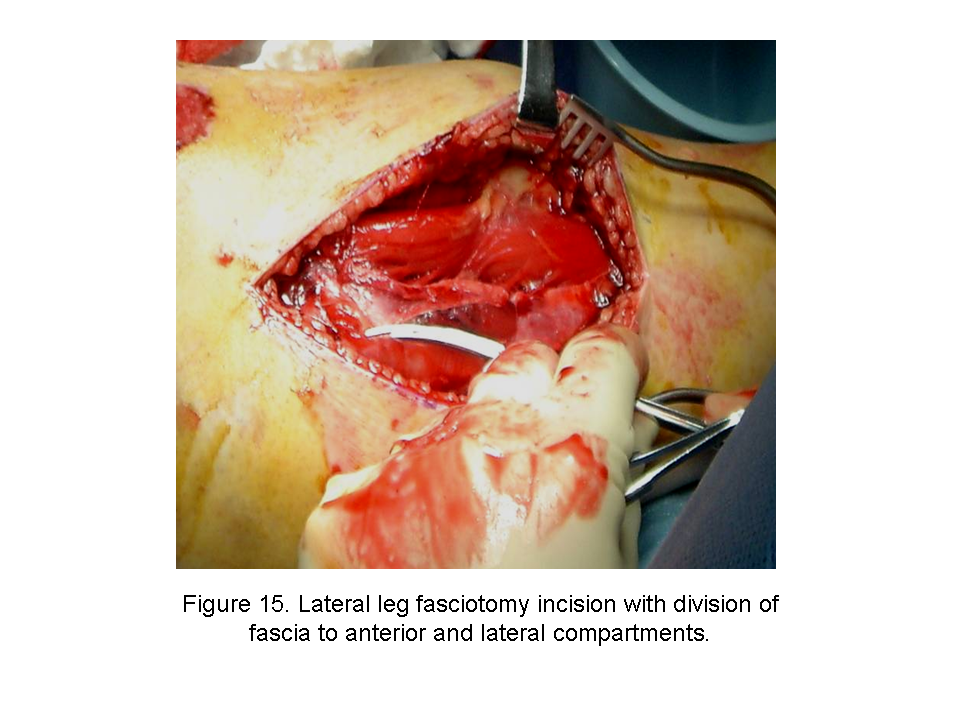{kind=link}
d. lateral compartment then released through this incision in line with fibular shaft, proximally toward fibular head, distally toward lateral mallelous
e. second incision made medially at least 2 cm medial to medial-posterior palpable edge of tibia (medial incision over or near subcutaneous surface of tibia is avoided, preventing exposure of tibia when tissues retract)
f. saphenous vein and nerve are retracted anteriorly
g. superficial compartment released through its length (see figure 16) and then the deep posterior compartment over the flexor digitorum longus is released (see figure 17)
{kind=link}
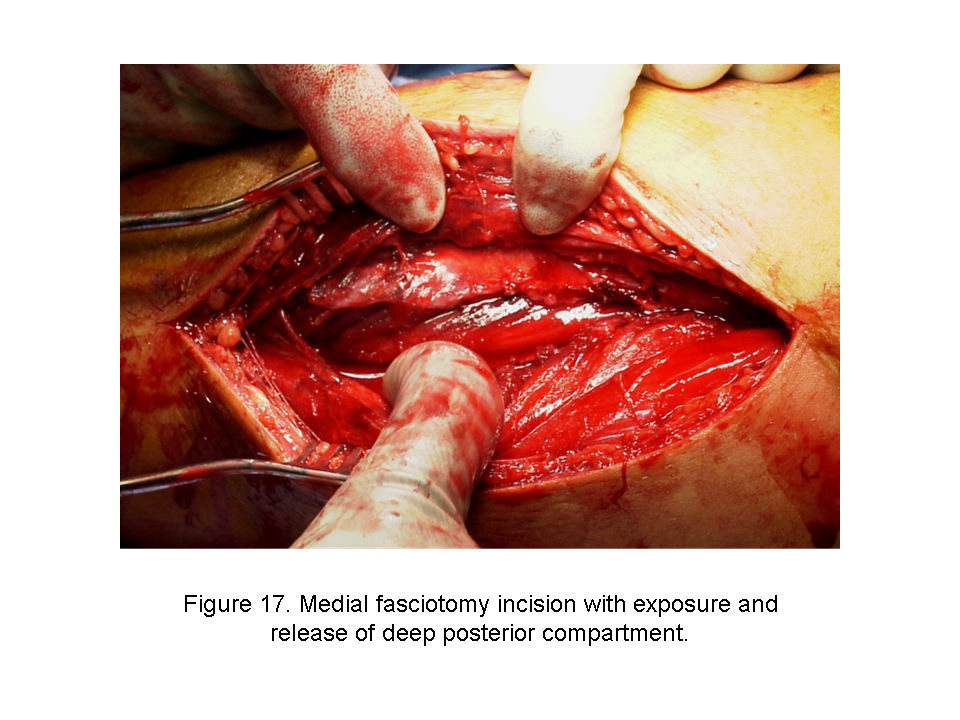{kind=link}
h. identify tibialis posterior and release its fascia
4. complications
a. weakness and dysfunction of affected muscle groups and transversing nerves
b. clawing of toes may also be commonly seen following compartment syndrome of deep posterior compartment
C. Foot
1. foot has five compartments
a. interosseous compartment (bounded by lateral first metatarsal medially, metatarsals and dorsal interosseous fascia dorsally, and plantar interosseous fascia plantarly)
b. lateral compartment (bounded by fifth metatarsal shaft dorsally, plantar aponeurosis laterally, and intermuscular septum medially)
c. central compartment (bounded by intramuscular septum laterally and medially, interosseous fascia dorsally, plantar aponeurosis plantarly)
d. medial compartment (bounded by inferior surface of first metatarsal dorsally, plantar aponeurosis extension medially, and intramuscular septum laterally)
e. calcaneal compartment (quadratus plantae muscle)
2. fasciotomy technique – dual dorsal incisions (see figure 18)
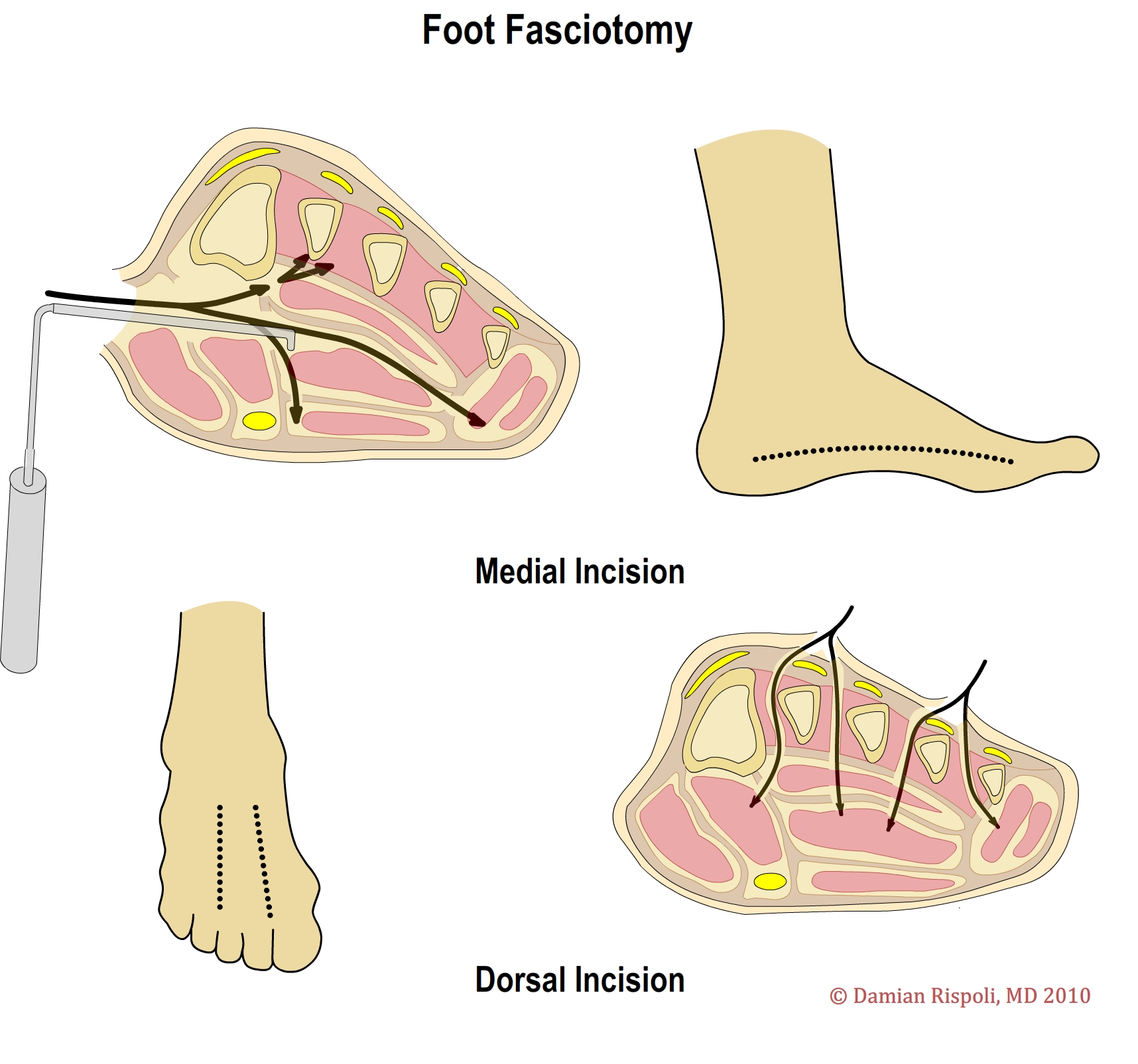{kind=link}
a. one incision placed slightly medial to second metatarsal, reaching between first and second metatarsals into medial compartment and between second and third metatarsals into central compartment
b. second dorsal incision made just lateral to fourth metatarsal, reaching between fourth and fifth metatarsals into lateral compartment
3. to spare dorsal soft tissue, single incision medial fasciotomy may be used (medial approach to foot is made through medial compartment, reaching across central compartment into interosseous compartment dorsally and lateral compartment releasing all the way across foot)
V. Fasciotomy Wound Management
A. After fasciotomy performed, wound must be debrided of all devitalized tissue (see figure 19)
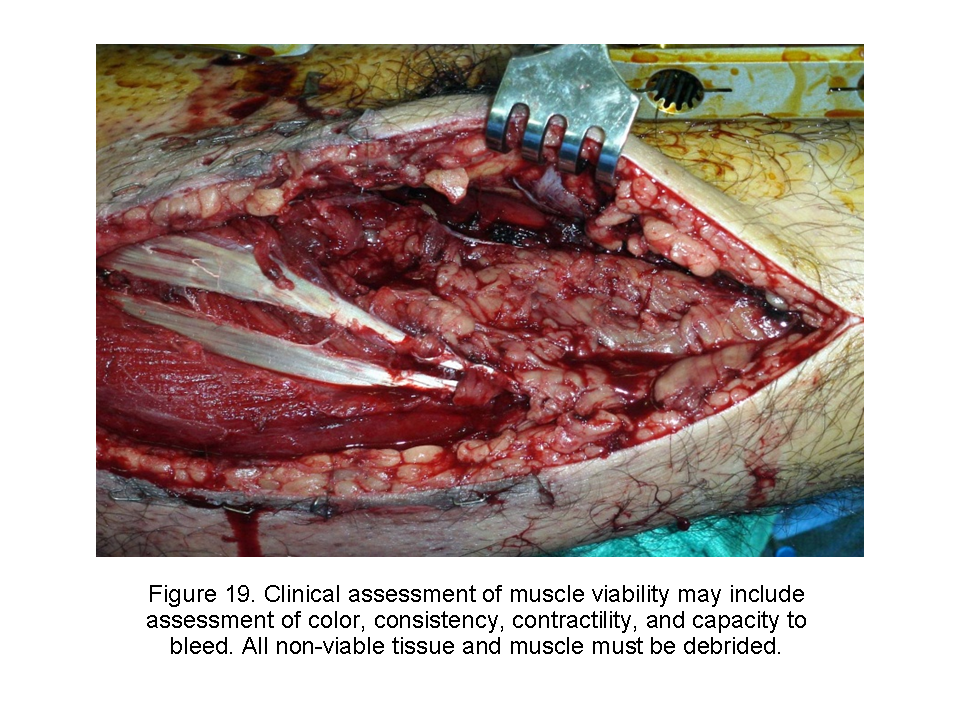{kind=link}
B. Treated as all war wounds without early closure and coverage with sterile dressing
C. Negative pressure wound closure devices useful in management of wounds
1. field expedient negative pressure closure devices can be created using available materials
a. laparotomy sponges
b. Jackson-Pratt drains
c. Ioban
D. Closure of fasciotomy wounds may be delayed until evacuation from austere environment can be coordinated (see figure 20)
{kind=link}
E. Closure options
1. delayed primary closure
2. healing by secondary intention
3. split thickness skin grafting or flap coverage
VI. Associated Vascular Injury
A. Pulses usually present in compartment syndromes
B. Absence of pulse should alert physician to presence of vascular injury and thus increased risk of developing compartment syndrome
C. Vascular injury is indication for compartment release in austere environment
The view(s) expressed herein are those of the author(s) and do not reflect the official policy or position of Brooke Army Medical Center, the U.S. Army Medical Department, the U.S. Army Office of the Surgeon General, the Department of the Army, Department of Defense or the U.S. Government.
Materials and support for The Disaster Preparedness Toolbox is provided by Lt Col. Ky Kobayashi, MD and Col. Benjamin Kam, MD.