- PreOp Planning
- most important step in reconstruction of any intra articular frx, is to expose the fracture w/o devasclarizing the fragments;
- treatment plan:
- open reduction;
- elevation of the depressed plateau;
- bone grafting of metaphysis;
- fixation of the fracture with cancellous screws
- butress plating of the lateral cortex;
- position:
- for optimal exposure, consider supine position, w/ a bolster under thigh, & table broken so that the knee is flexed 90 deg;
- this position allows increased exposure submeniscally;
- Surgical Approach:
- consider a longitudinal lateral parapatellar approach;
- elevate anterior compartment muscles off proximal tibia, exposing tibial flare and split frx;
- trace frx is to joint line and enter joint thru transverse sub-meniscal interval;
- if needed, transect attachment of anterior horn of meniscus;
- elevate meniscus superiorly to expose intra-articular frx segment;
- if the anterior compartment is tight, consider limited fasciotomy to avoid compartment syndrome;
- Exposure of Depressed Segment:
- split frx is hinged open anteriorly (like a book) to expose depressed joint surface;
- insert an osteotome below the subchondral cancellous fragments and gently tap the osteotome until it comes to rest along the posterior
tibial cortex;
- use the posterior cortex as a fulcrum for the osteotome and lever it upwards to lift all of the frx fragments "en mass" until they are
congruent with the joint line;
- the mistake to avoid is to attempt to individually disimpact frx fragments, since this results in multiple separate pieces which cannot be
held congruent at the joint line;
- elevated segment may be supported w/ K wires (consider biodegradable);
- metal wires can be inserted from the opposite (medial) condyle in order to maintain the elevation of the depressed fragment
temporarily, until the split fragment is firmly reduced;
- absorable K wires can be inserted from both the medial and lateral sides, to form a carpet configuration;
- apply bone graft from below;
- this surface is elevated to appropriate level & defect is filled w/or local cancellous bone or allografts;
- Implants:
- at this point, the frx has essentially been turned into a type I frx;
- w/ minimal comminuation and good bone stock, consider 6.5 mm cancellous screws w/ or w/o washers;
- if cannulated screws are used, these are inserted over K wires;
- if split fragment is not comminuted, 2 or 3 cancellous screws are inserted parallel to & > 1 cm distal to articular surface;
- an additional, cortical anti-glide scrw w/ washer is inserted distally;
- in older patients, w/ osteoporotic bone, one cannot rely on lag screws alone to prevent redisplacement of fragments;
- a butress plate is almost a must;
- a comminuted frx, requires an L or T shaped buttress plate;
- another indication, for butress plating is assoc subcondylar frx;


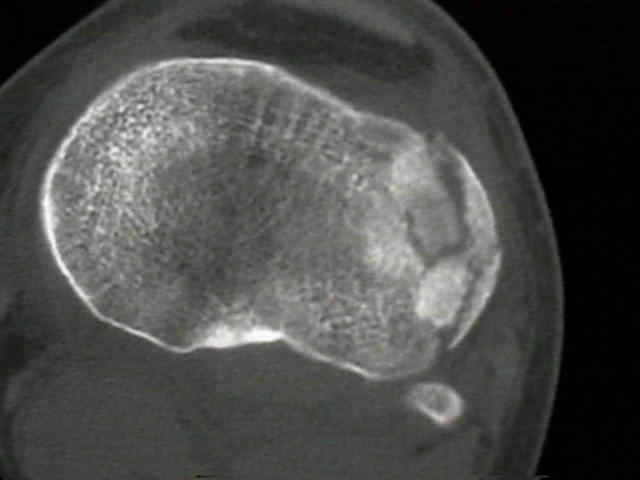
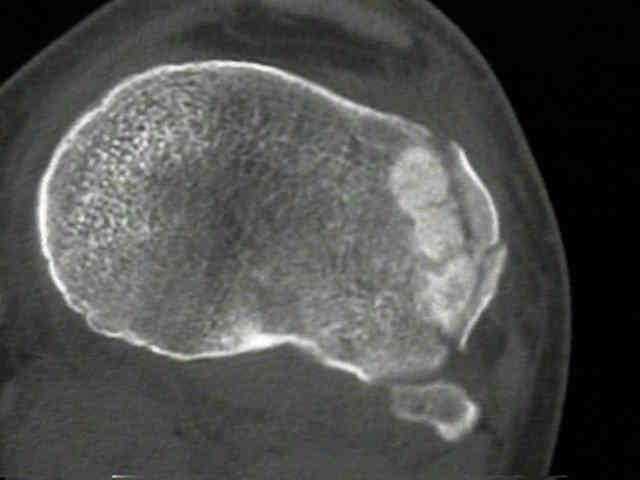
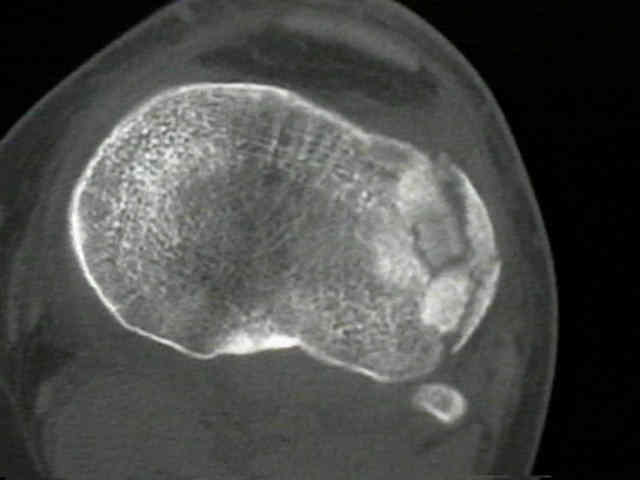
- Case Example:
- 30 year old male who fell during a soft ball game.
- as the axial view clearly shows, there are several intra-articular fragments which are impacted into the metaphyseal bone;
- as expected, complete anatomic restoration of these multiple articular fragments could not be achieved