
 Images kindly provided by Donald Serafin M.D., Duke University Medical Center
Images kindly provided by Donald Serafin M.D., Duke University Medical Center
- Discussion:
- epineural repair is currently the gold standard for repair, as no prospective studies have indicated than fasicular repair is superior;
- it is probably most indicated w/ pure sensory or pure motor nerves;
- Technique:
- expsure: see: Phalangeal Incisions:
- debridement:
- zone of injury must be defined;
- damaged nerve ends are sharply debrided to clean edge of fasicles;
- to overcome small defects that occur w/ nerve transection and debridement, the nerve ends must be mobilized to some degree;
- rotational alignment:
- an attempt is made to align group fasicles and/or longitudinal epineural vessels;
- if nerve ends are retracted, the ends can be approximated by transfixing the epineurium at each end with small straight needles,
which are then driven into soft tissue;
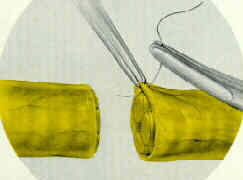
- epineural repair:
- initially two sutures spaced 180 deg apart are inserted;
- with small nerves, only two or three sutures (8-0) may be required, where as with larger nerves, up to 6 sutures may be reqired;
- microvascular forceps lift epineurium and needle is driven thru epineurium;
- generally only the epineurium is included in the repair;
- on some occassions, such as median nerve lacerations at the wrist, the internal epineurium can be included in the external
epineural stitch inorder to better oppose group fasicles;
- after the suture is tied, one end is left long, to facilitate further repair;
- 2nd suture is placed 120 deg apart, again leaving one end long;
- remaining anterior sutures can now be applied;
- now one suture is passed beneath and around nerve, and w/ gentle traction the nerve should twist around 180 deg;
- traction is maintained by using microsurgical clips which are applied to soft tissue;
- remaining sutures are applied;
- management of tension at nerve site repair