
- See: Peroneus Longus / Peroneus Brevis:
- Discussion:
- acute dislocation occurs by sudden forced dorsiflexion w/ concomitant eccentric contraction of the peroneal muscles;
- classic teaching that the tendon dislocation occurs from a combination of dorsiflexion and eversion (like skiing), where as other authors feel
that the injury occurs from dorsiflexion and inversion (which accounts for its association with ankle instability);
- chronic peroneal tendon dislocation is often associated w/ recurrent ankle sprains, which lead to incompetency of peroneal retinaculum, and
subsequent tendon subluxation;
- patho-anatomy:
- at the level of the ankle joint, the peroneal tendons lie in a groove in the posterior fibula;
- grove is present in (82%) fibulas, a transverse flat surface in 19 (11%), and a convex surface in 13 (7%);
- average width of sulcus, when present, is 6 mm;
- lateral border of the posterior fibular surface may form a bony ridge (2-4 mm) augmenting the sulcus;
- peroneus longus courses posterior to the brevis tendon, and then both tendons pass thru the common peroneal synovial sheath,
about 4 cm proximal to the lateral malleolus;
- synovial sheath passess through a fibro-osseous tunnel that is stabilized by the superior peroneal retinaculum and by calcaneofibular ligament;
- superior peroneal retinaculum:
- primary constraint to peroneal tendon subluxation;
- retinaculum is formed as a confluence of superficial fascia, and sheath of peroneal tendons, and periosteum of distal fibula (about 2 cm proximal to fibula tip);
- formed from thickening of fascia that arises off the posterior margin of distal 1-2 cm of the fibula and runs posteriorly to blend with the Achilles tendon sheath.
- synovial sheath passes behind the distal fibula (retromalleolar sulcus), and the depth of the sulcus may be related to propensity for peroneal subluxation;
- w/ peroneal tendon dislocation there is stripping of the periosteum from the lateral malleolus which is in continuity w/ superior peroneal retinaculum;
- result is the creation of a false pouch posteriorly (similar to the false pouch created by a shoulder Bankhart lesion);
- associated findings:
- anterolateral instability of the ankle is associated with laxity of the superior peroneal retinaculum;
- superior peroneal retinaculum is a secondary constraint to anterolateral ankle instability;
- degenrative changes and longitudinal splitting in the peroneus brevis tendon;

- Exam:
- there will be tenderness posterior to the lateral malleolus;
- subluxation of the peroneal tendons may be provoked by having the patient dorsiflex the foot from a position of dorsiflexion and eversion;
- look for a prominence of the tendon w/ dorsiflexion and internal rotation;
- w/ chronic peroneal tendon subluxation, there will often be signs of ankle instability;
- w/ a questionable exam, consider a diagnostic lidocaine injection into the peroneal tendon sheath;
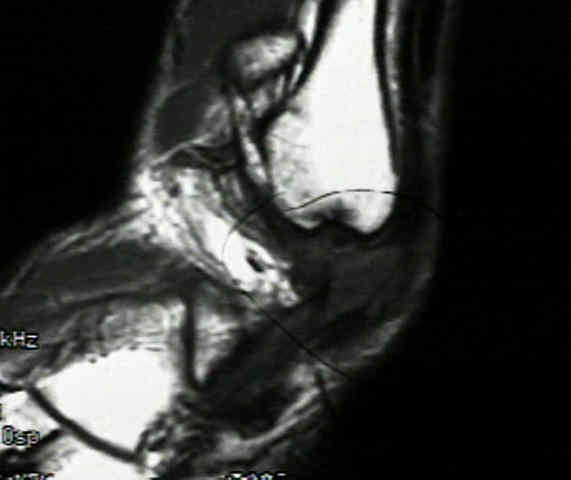
Imaging:
- need to assess mortise view of the ankle;
- look for shell-like avulsion fracture of the lateral malleolus (which indicates disruption of the peroneal retinaculum) and dislocation of the peroneal tendons;
- Tenograms and CT may be used, but MRI is of greatest value in evaluating soft tissue structures
- Non Operative Treatment:
- ensure that the tendons are reduced before immobilization;
- place in plantar flexion in slightly inverted below knee cast for 6 wks
- note that conservative treatment for acute injuries in active young athletes, generally has a relatively high recurrence rate (50%);
- Surgical Treatment:
- in active patients, surgical fixation of the disrupted sheath is treatment of choice.
- Surgical Options: peroneal groove deepening, tenoplasty, or bone block;
*- Groove Deepening with SPR repair
- if performed with care can preserve the periosteal flaps and help secure tendon sheath to posterior fibula
- Kollias and Ferkel (1997) 95% success rate
- Mendicino et al (2001) 100% success rate
- Surgical Technique
- osteotomize distal posterior fibula leaving medial side hinged
- curette underlying cancellous bone
- reinsert flap into deepened bed
- Advantages
- correct groove deficiency
- maintain cartilaginous gliding layer
- rare recurrence, all reinforced SPR simultaneously
- Disadvantages
- tendon irritation on bony edges, failure to correct dislocation pouch
- tenodesis should be performed 3-4 cm above the fibular tip and 5-6 cm below the fibular tip;
- in the Singapore operation, the false pouch is obliterated by suturing down the superior retinaculum to the posterior fibula;
- a secure repair, requires drill holes to be made in the distal fibula;
- in some cases, a slip of Achilles tendon may be required to augment the repair;
- hazards: note that the sural nerve lies about 1 cm distal to the distal end of the fibula
Tendon injuries about the ankle resulting from skiing.
Static or dynamic repair of chronic lateral ankle instability. A prospective randomized study.
Recurrent dislocation of the peroneal tendon.
Traumatic dislocations of the peroneal tendons.
Acute rupture of the peroneal retinaculum.
Dislocation of the peroneal tendons long term surgical treatment.
Dislocation of the peroneal tendons.
Sliding fibular graft repair for chronic dislocation of the peroneal tendons.
Traumatic Peroneal Tendon Instability
Superior peroneal retinaculoplasty: a surgical technique for peroneal subluxation.
Current Concepts Review: Peroneal Tendon Subluxation and Dislocation