
- Technique:
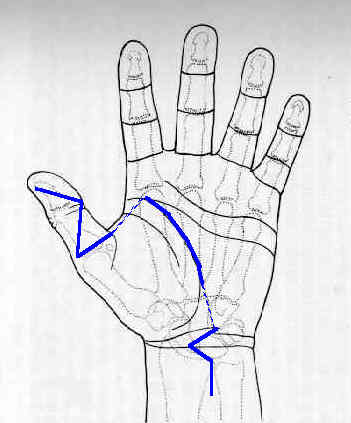
- Brunner Incision is made extending from distal phalanx of thumb to the MP crease;
- digital nerves and vessels are identified (protected by Grayson's ligament);
- dissection procedes down to the oblique and transverse flexor tendon sheaths;
- the proximal and distal aspect of each sheath is identified;
- clear the distal tendon remnants from the tendon sheath;
- attempt to located the torn edges of the FPL tendon, but note that the tendon usually retracts proximally to a point
proximal to the transverse carpal ligament;
- proximal tendon retraction can occur because their is no vinculum, and no lumbrical to proximally tether the tendon;
- make a second incision over the wrist, 4-5 cm in length longitudinally just proximal to the transverse proximal ligament;
- be aware that the median nerve lies directly beneath the superficial fascia;
- thru this incision, use a right angle to systematically elevate the flexor tendons, (FDS, FDP, FPL) until the FPL is identified;
- the FPL is pulled proximally out of the wound;
- break up proximal adhesions over the proximal FPL muscle belly;
- Bunnel suture is inserted using PDS (allowing future pull out);
- preparation for tendon advancement:
- w/ the tendon is placed under tension, and drawn toward the thumb IP joint;
- the tendon length deficit is measured with a ruler;
- using a 15 blade scapel, a longitudinal incision is made down the middle of the exposed tendon, a distance 2-3 cm longer than
the measured length deficit;
- complete the "Z" step cuts;
- procede to the "pull thru" portion of the case, with the plan that ultimate tendon tension can be determined at the end of the case;
- the flexor tendon sheaths are dilated;
- a tendon passer is inserted from distal to proximal and grasps the pull out suture;
- the tendon passer (and suture) is pulled distally, and the tendon is delivered thru the tendon sheaths;
- note that the FPL tendon sheaths are often tight, and great care is required to prevent the tendons from becoming "bunched up"
at the tendon entrance;
- pull thru technique:
- using straight free needles, each limb of the Bunnel suture is passed on either side of the proximal phalanx so that the needles
exit just proximal to the each corner of the nail;
- tie the sutures over soft rubber and a button;
- at this point the distal wound should be closed, since wound closure will be difficult once the tendon is repaired under tension;
- tendon advancement;
- the tendon edges of the "Z" cut are overlaped aproximately 2-3 cm, and are held togehter w/ one or two 25 gauge needles;
- the optimal tension on the tendon will allow the tenodesis effect, which causes the thumb IP joint to relax w/ wrist flexion
and to flex with wrist extension;
- if tension is too tight, the thumb will pull over to the index finger, as the wrist is extended;
- often the proper tension relationship is determined by stretching the muscle to its maximal length and then allowing it to retract
50%;
- tendon edges are sutured together using 4-0 Ethibond horizontal matress sutures;
- reconfirm an optimal tenodesis effect;
- close the proximal wound