

 - Discussion:
- Discussion:- by definition, invovles RTC tears of more than 5 cm and involves more than than one tendon;
- further, massive tears cannot be repaired w/o excessive tension after lysis cuff adhesions and release of the coracohumeral ligament; (see cuff mobilization)
- Management:
- rotator cuff repair: / arthroscopic repair
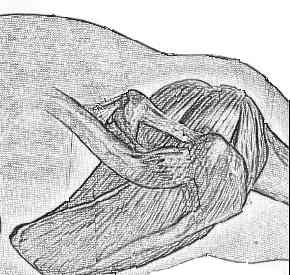
- assessment of size of rotator cuff tear:
- infraspinatus insertion zone was identified by laying 2 branches of forceps over scapular spine so that forceps were in line with fibers of cuff;
- fibers coming from a level inferior to the scapular spine are infraspinatus fibers;
- teres minor insertion was identified by locating its insertion on the respective tubercle, which lies inferior and slightly medial to infraspinatus insertion;
- cuff mobilization
- medialization of the supraspinatus tendon: (restoration of foot print)
- indicated for situations in which the rotator cuff cannot be adequately mobilized;
- instead of reattachement of cuff to greater tuberosity, the cuff is re-attached to the a groove created on anatomic neck or on humeral head;
- as noted by Liu J, et al. 1998, about 1 cm of medialization may be acceptable but 17 mm of supraspinatus medialization will result in a significant reduction in the moment arm;
- references:
- Biomechanical Effect of Medial Advancement of Supraspinatus Tendon. A study in cadavera.
- Arthroscopic treatment of massive rotator cuff tears. Clinical results and biomechanical rationale.
- Massive Tears of the Rotator Cuff
- biceps tendon:
- references:
- Isolated arthroscopic biceps tenotomy or tenodesis improves symptoms in patients with massive irreparable rotator cuff tears.
- Arthroscopic debridement of irreparable massive rotator cuff tears -- a comparison of debridement alone and combined procedure with biceps tenotomy
- Arthroscopic biceps augmentation for avoiding undue tension in repair of massive rotator cuff tears
- Bridging the gap in immobile massive rotator cuff tears: augmentation using the tenotomized biceps
- The role of the biceps tendon in massive rotator cuff tears.
- Biceps Augmentation
- acromioplasty and cuff debridement:
- in well selected patients, cuff debridement and acromioplasty can lead to a significant decrease in pain and increase in ROM;
- good prognostic indicators are an intact anterior deltoid and an intact long head of the biceps;
- poor prognostic factors include non-functioning anterior deltoid and previous acromioplasty and attempted RTC repair;
- if an acromioplasty is indicated, then attempt to leave the CA ligament intact and the acriomplasty should be conservative;
- some feel that excision of the CA ligament and an agressive acriomplasty may lead to postop weakness and/or glenohumeral subluxation;
- w/ a potential irrepairable cuff tear, consider leaving the CA ligament intact - intact ligament helps prevent superior migration of humeral head;
- relative contra-indications:
- superior migration of humeral head;
- as noted by Gartsman GM (1997), all patients w/ radiographic superior migration of the humeral head had a poor result;
- deficient deltoid, subscapularis, and/or teres minor (either by clinical exam or by MRI) are more likely to lead to poor results;
- technical considerations:
- after performing an appropriate acromioplasty, debride all avascular tissue;
- when cuff is not repairable, ensure that there is no soft tissue remanants of the cuff which could be impinged between the humeral head and acromion;
- when an exostosis on the greater tuberosity is present, it should be removed - apply bone wax to prevent recurrance;
- ensure that the deltoid is firmly anchored to the remaining acromion;
- some recommend preservation of the biceps tendon whenever possible, others will consider excision of the tendon if it is loose or frayed;
- references:
- Debridement of degenerative, irreparable lesions of the rotator cuff.
- Massive, Irreparable Tears of the Rotator Cuff. Results of Operative Debridement and Subacromial Decompression.
- Superior humeral dislocation. A complication following decompression and debridement for rotator cuff tears.
- reverse acromioplasty / tuberoplasty:
- shoulder hemiarthroplasty in the rotator cuff deficient patient:
- references:
- Results of arthroscopic decompression and tuberoplasty for irreparable massive rotator cuff tears.
- Reversed arthroscopic subacromial decompression for symptomatic irreparable rotator cuff tears: mid-term follow-up results in 34 shoulders.
- Reversed arthroscopic subacromial decompression for massive rotator cuff tears.
- latissimus dorsi transfer:
- references:
- Latissimus dorsi transfer for the treatment of massive tears of the rotator cuff. A preliminary report.
- Latissimus dorsi transfer for the treatment of irreparable tears of the rotator cuff.
- Transfer of the Latissimus Dorsi Muscle After Failed Repair of a Massive Tear of the Rotator Cuff. A two to five-year Review
Long-Term Outcome After Pectoralis Major Transfer for Irreparable Anterosuperior Rotator Cuff Tears
Advancement of the supraspinatus muscle in the repair of ruptures of the rotator cuff.
Arthroscopic suprascapular neurectomy for the management of severe shoulder pain