
- Salter Harris Type II Fractures:
- 80% of type II fractures can be managed non operatively;
- displaced SH type-I or II frx are reduced closed w/ pt under GEA;
- reduction is obtained mainly by traction rather than manipulation;
- 90 % traction, 10 % manipulation;
- knee may require flexion for reduction, however, too much flexion may risk vascular comprimise;
- anterior displacement:
- may be associatted w/ vascular insufficiency, as the popliteal artery is injured by the distal femoral metaphysis;
- reduction of these frx is facilitated by having patient in the prone position and flexion of knee to 90 deg, utilizing the intact anterior periosteum;
- treated w/ single leg spica cast in slight to moderate knee flexion for 6 weeks;
- posterior displacement is treated w/ single leg spica cast in extension;
- note that casting the patient in extension may be more painful than flexion, and therefore, if adequate reduction is achieved w/ slight flexion, then casting in extension is not necessary;
- if reduction is not possible, consider interposed soft tissue;
- following reduction of a displaced frx, determine whether frx is stable or unstable (as determine from flouroscopy);
- if the fracture is unstable then some form of fixation is necessary;
- Operative Rx: SH II Frx:
- percutaneous screw fixation:
- mainly indicated for type II fractures with a large Thurstan Holland metaphyseal spike, which will accomodate one or two screws;
- obviously screws cannot cross the fracture site;
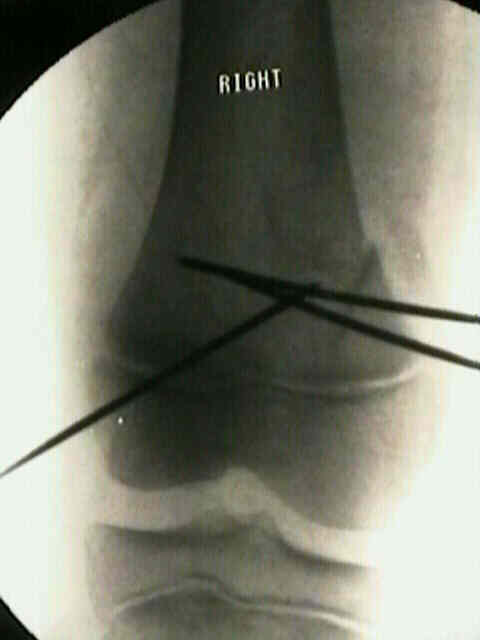
- percutaneous pinning w/ smooth Steinmnan pins placed through metphyseal fragment, parallel to the
epiphysis is recommended for displaced or angulation frx;
- optimally fixation will not cross the physis, however, transmetaphyseal pins may be required for unstable type I frx or type II frx w/ a short metaphyseal fragment;
- in this case, pins should be directed through the center of the physis in order to minimize any angulatory deformity that might result from physeal bar formation;
- in general, pins are cut beneath the skin inorder to avoid infection and subsequent joint sepsis;
- if acceptable reduction is not possible, then ORIF is required;
- the block to reduction may be a medial periosteal flap;
- following internal fixation, a long leg cast is applied with slight flexion;
- case example:
- 9 year old female who was pinned between a car bumper and a brick wall, sustaining bilateral distal femoral physeal frx;
- open reduction was required along w/ internal fixation w/ Steinman pins;








- Complications: Growth Plate Arrest:
- limb length descrepancy of more than 1 cm may occur in over 40%.
- angular deformities may occur in a third of patients
Traumatic injuries of the distal femoral physis. Retrospective study on 151 cases.