
- History:
1963 – Maurizio described the association of patellar tendonitis with jumping
1973 – Blazina, et al. coined the term “jumper’s knee”
1978 – Mariani, et al. and Roels, et al. widened the term “jumper’s knee” to include pathology of the patellar tendon at the tibial tuberosity
1986 – Ferretti outlined the epidemiology of jumper’s knee
- Jumper's knee.
- Jumper's knee.
- Patellar tendinitis (jumper's knee).
- Epidemiology of Jumper's Knee
- Discussion:
- inflammation of patellar tendon second to repetive trauma (jumping sports);
- seen in athletes involved in running, jumping, and kicking sports;
- occurs usually in skeletally mature adults, Age range 16 to 40 years, males slightly > females
- excessive foot pronation and running hills can exacerbate these symptoms;
- Etiology:
Intrinsic Factors (Ferretti (1986))
- Sex, Age, knee alignment, Q angle, patella position, tibial/femoral rotation, knee stability, morphotype
- HOWEVER, studies have found NO relationship with these factors
- Implied relationship with hamstring and quadriceps tightness (Writvrouw, et al. (2001)) and knee flexion angle at the time of stress (Richards, et al. 1996)
Extrinsic Factors (Ferretti (1986))
1) Hard playing surfaces Cement 38% Parquet 4% Linoleum 23%
2) Length of training sessions
Bassett, et al. (1990) believed in a triad of extrinsic factors:
1) magnitude of applied force
2) duration of load
3) angle of the knee flexion during stress
- Epidemiology of Jumper's Knee
- Knee joint dynamics predict patellar tendinitis in elite volleyball players.
- Intrinsic risk factors for the development of anterior knee pain in an athletic population. A two-year prospective study.
- Magnetic resonance imaging of knee trauma.
- Pathogenesis:
- Extensor mechanism stress, acceleration/deceleration, jumping/landing, extrinsic overload of the tendon
- Microtears within the tendon matrix, rare occurrences of rupture
- Patellar impingement theory
- Impingement of the inferior patellar pole against the patellar tendon during knee flexion, Often resulting from a “long inferior patellar pole”
- Controversy
- Johnson, et al. 1996 (JBJS) found impingement of the interior pole at 60 degrees of knee flexion
- Schmid et al. 2002 suggested that there was no biomechanical evidence of impingement in their series
- Almekinders and Shalaby 1999 found evidence of a “long inferior pole” in symptomatic patients, but this abnormality did not always correlate to the region of involved tendon
- Many surgeons resect the infrapatellar pole during both open and arthroscopic debridement of patellar tendonitis
The effect of continuous passive motion on wound-healing and joint mobility after knee arthroplasty.The effect of continuous passive motion on wound-healing and joint mobility after knee arthroplasty.
- Histopathology:
- Evidence of chronic overuse syndrome, No evidence of acute inflammation
1) Degeneration: mucoid degeneration, fibrinoid necrosis, pseudocyst change, and myxomatous degeneration
2) Regeneration: neovascularization, increased cellularity, chronic inflammation, angiofibroblastic tendinosis
classification: (Blazina, et al (1973), Roels, et al (1978))
- phase I: pain only after activity;
- phase II: pain/discomfort during activity, but does not interfere w/ participation;
- phase III: pain both during & after participation, which interferes w/ competition;
- phase IV: complete tendon disruption.
- Jumper's knee
- Patellar tendinitis (jumper's knee).
- Exam:
- Perform exam with knee in full extension
- Bassett Sign:
- Tenderness to palpation with knee at full extension and patellar tendon relaxed
- Non-tender with knee in flexion and patellar tendon taut
- Quadriceps atrophy
- Quadriceps and hamstring tightness
- Knee effusion is rare
- Ligaments usually stable
- Various biomechanical derangements may be present on exam
- excessive foot pronation;
- ie. Malalignment, patellar hypermobility, patella alta/baja, tibial/femoral rotation, etc.
- However, no correlation with jumper’s knee exists for these intrinsic factors (Ferretti 1986)
- X-ray:
- in adolescents, sclerosis, decalcification, and fragmentation at the inferior
pole of the patella is referred to as Sindig-Larsen-Johanssen disease;
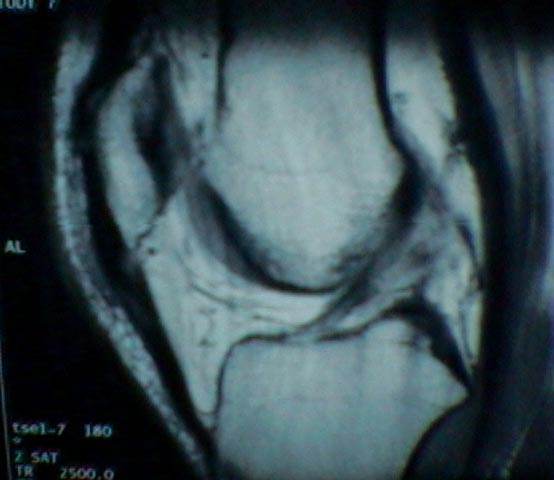
- MRI or Ultrasound: may confirm the diagnosis; Bone scan ~ 29% false-negative rate

- Non-Operative Treatment:
- Ice, NSAIDs, Bracing & Strapping, Activity modification: Rest & PT
- Steroid injection – controversial, but not recommended
- Surgical Intervention:
- Indications
- High profile athlete
- Failure of 6 months non-operative therapy
- Tendon rupture
- Open Tendon debridement
-Local anesthesia without tourniquet, Longitudinal or transverse incision,
-Some remove central tendon, Some preserve superficial tendons and resect deep fibers
-Avoidance of competition: 4 to 6 months
- Pole excision with reinsertion of tendon
- Realignment
- Arthroscopic Tendon and Fat Pad debridement
-Local anesthesia with sedation, localize the lesion with 18 ga. spinal needle – maximal tenderness and MRI correlation
-Debridement of the inflamed fat pad and diseased tendon – down to healthy fibers
-Debridement of enthesis and inferior pole of patella
- Literature Review of Operative Treatment Results
- Orava et al 1986 examined success of open debridement
-150 athletes over 5 year period with Dx, 34 treated with open debridement, Mean F/U 4.5 years (6 months - 8 years)
-23 with complete relief (~68%), 9 with pain at exercise (~26%)
- Colosimo and Bassett (1990) reviewed their cases of open debridement
-200 athletes over 20 year period with Dx, 67 surgically treated with open debridement
-54 with complete relief (~80%) by 12 months, Focal area of tendinosis required complete removal
- Coleman et al 2000 compared open vs arthroscopic (Retrospective)
-25 vs 23 patients (~4 year f/u)
-similar symptomatic relief and outcome, 50% return to prior level of competition in each group
-arthroscopic group returned to sport ~4 months earlier than the open debridement group
- Jumper's knee. Diagnosis and treatment
- Associated syndromes:
Sinding-Larsen-Johansson Disease:
- osteochondrosis of the inferior pole of the patella
- presents as anterior knee pain in the active adolescent
- usually resolves with skeletal maturation
Osgood-Schlatter Disease:
- partial avulsion of the tibial tubercle
- presents as tenderness at the tibial prominence in active adolescents
- usually resolves with rest
Etiology, histopathology, and outcome of surgery in achillodynia.
Long-term prognosis for jumper's knee in male athletes. A prospective follow-up study.
Patellar Tendinosis. A Follow-up Study of Surgical Treatment.