
- Discussion:
- 11% of cases
- occurs following significant trauma, produces sudden onset of pain severe enough to prevent weight bearing;
- pts usually report minimal or no previous symtoms;
- Treatment:
- reduction vs. traction:
- gentle repositioning can reduce the deformity of an acute slip.
- gradual traction may be safer than acute manipulative reduction;
- full reduction may lead to avascular necrosis of femoral head;
- manipulation should not be attempted for an acute slip that has been present for more than 2 weeks.
- pin placement:
- in acute slips, two or three threaded pins are inserted across epiphysis to prevent further slippage;
- Complications:
- avascular necrosis:
- risk factors:
- severity of slip
- reduction of slip
- location of pins (questionable significance);
- need to avoid anterolateral cortex;
- number of pins (questionable significance);
- risk of AVN is approx 20-50% w/ attempted reduction vs. less than 5% w/o reduction;
- case example:
- 12 yo female w/ acute slip who achieved significant reduction w/ gentle traction on fracture table




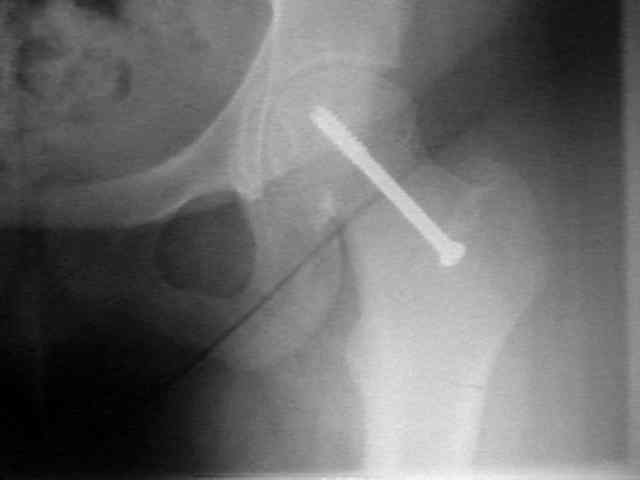
Age 12 (preop) Early postop films Age 14 (no AVN)
Acute slipped capital femoral epiphysis: the importance of physeal stability.