
- results from supination-adduction fracture (Weber A)
- adduction forces result in a vertical fracture of the medial malleolus at the junction of the plafond and malleolus;
- transverse fibular frx or tear of lat collat occurs concomitantly;
- medial soft tissues are intact so that interpostion is not problem;
- main problem is comminution at medial corner of mortise;
- plafond may be comminuted w/ impacted fragments, leading to varus tilt of mortise & post traumatic arthritis;
- Surgical Technique:

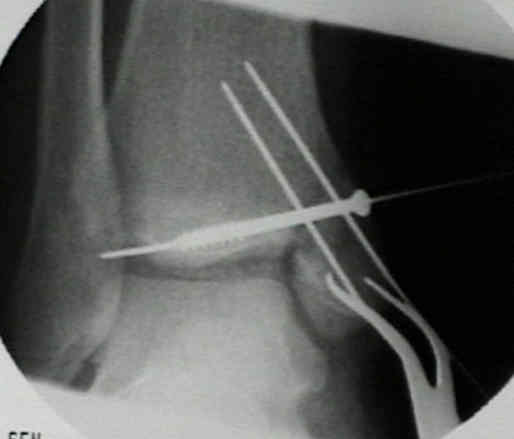
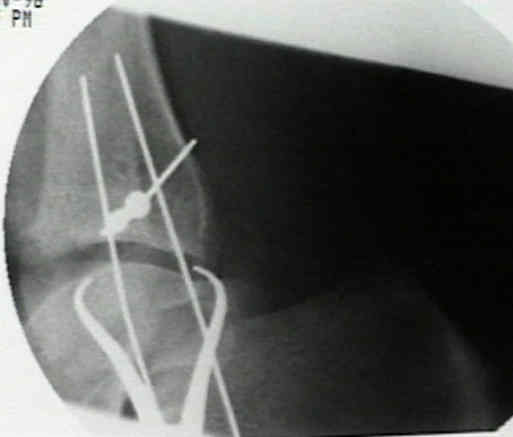


- vertical frx of medial malleolus are fixed w/ cancellous screws placed perpendicular to the fracture site;
- usually 2 cancellous screws are required;
- washers may be needed because of thinner medial cortex;
- when choosing site of screw insertion, avoid areas likely to produce further comminution of the fragment;
- screws should be seated in dense bone of the central distal tibial metaphysis and thus should be approximately 40 mm long;
- do not attempt to anchor them in the far cortex, which is too thin to provide much purchase;
- Comminution:
- medial surface should be inspected for articular crush of tibial surface or talar dome;
- w/ joint congruity, impacted fragments need to be reduced w/ bone graft applied to metaphyseal defects;
- if proximal portion of vertical frx is comminuted, butress plate may be required;
- w/o use of butress plate a varus deformity of talus may develope;
- plate may be small DC plate, one third, a T or clover leaf plate will suffice
Comparison of Surgical Techniques of 111 Medial Malleolar Fractures Classified by Fracture Geometry.