
 - Techique:
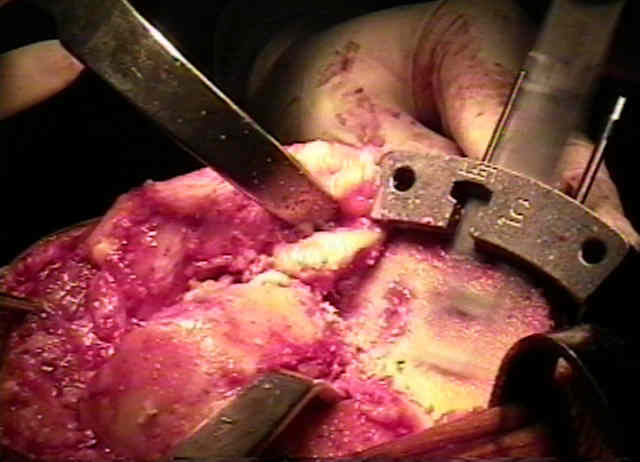
- Techique: - preparation and exposure for the proximal tibial cut:
- hyperflexion of the knee to allows the vessels to fall more posteriorly;
- curved knee retractors are positioned anterior to mid-coronal plane, so that patella tendon and MCL will not be injured;
- inadvertent transection of the lateral patellar tendon may occur w/ inadequate retraction during the proximal tibial cut;
- homan retractor may be placed behind posterior tibia and levered off of distal femur, which allows tibia to be translated anteriorly;
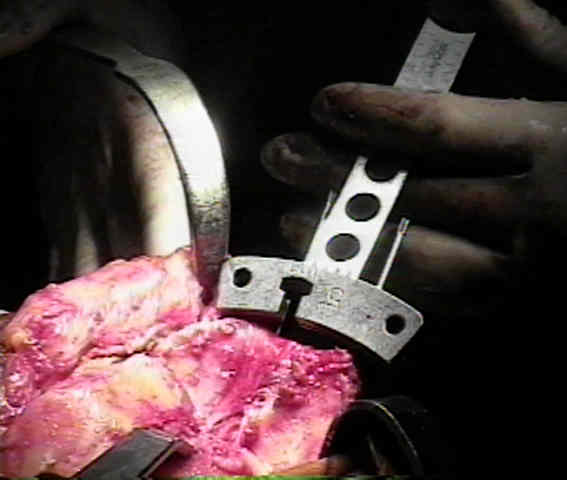
- extramedullary guides:
- depth of the tibial cut (avoid lowering of the joint line)
- posterior slope:
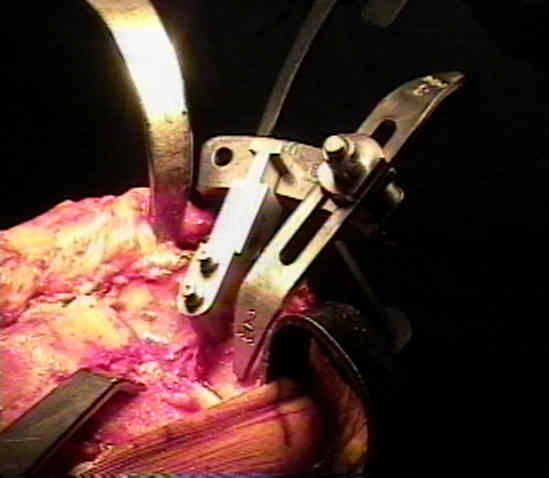
- rotation of tibial component:
- mechanisms can be used to avoid tendency to internal rotation;
- look down on tibial plateau & cutting jig w/ knee in flexion;
- face of jig should be parallel to plane of the femoral condyles;
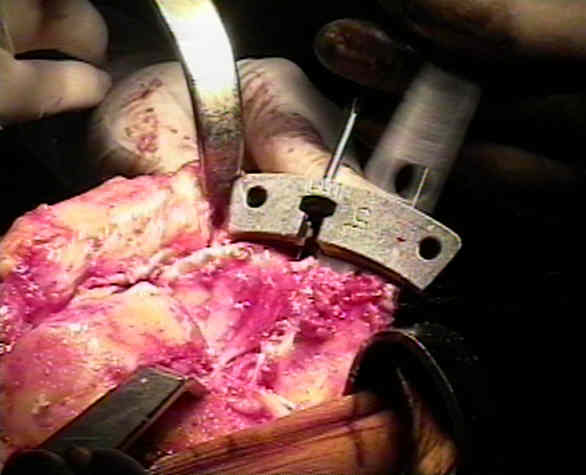
- plane of resection of the mechanical axis:
- after fixing tibial cutting jig in place, gentily flex and extend knee while watching that axis of cutting jig is parallel to axis of rotation of knee;
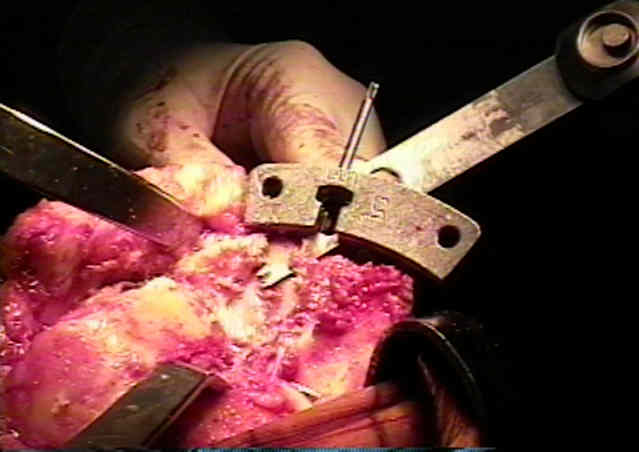
- current techniques involve making tibial cut parallel to the tibial anatomic axis (and cutting distal femur at 5-7 deg to its anatomic axis);
- this reduces the probability of inadvertent excessively varus cut and thus the likihood of varus alignment of the limb;
- as its easier to cut right angles than 3 deg off right angle & varus error in tibia is most common error w/ significant implicantions,
most techniques call for resection of upper tibia at 90 deg to its long axis;
- valgus errors are well tolerated while varus errors are not;
- original PCA technique involved making the proximal tibia in 3 deg of varus in relation to its longitudinal axis;
- this means that distal femoral cut must be approx 9 deg of valgus in relation to anatomic axis of femur to have overall mech axis of 0 deg;
- hazards:
- peroneal nerve:
- at the level of tibial bone resection, the common peroneal nerve lies superficial to the lateral head of the gastrocnemius;
- mean distance from the bony posterolateral corner of the tibia to the nerve was 1.49 cm, with no distance less than 0.9 cm.
Injury to the popliteal artery and its anatomic location in total knee arthroplasty