
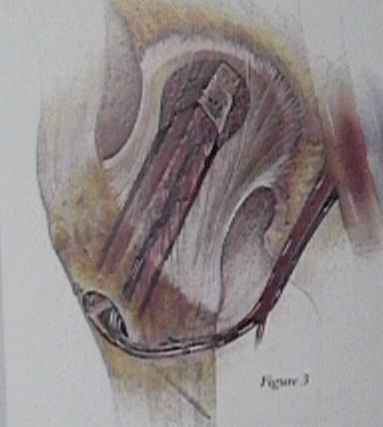
- Technique: The fibula is approached through a lateral incision simultaneous to the hip approach. The surgeon stands on the posterior side. The incision is planned on a line directly over the fibula. The fibular bone cuts will be 15 cm apart with the distal cut at 10 cm proximal from the distal fibular tip. The sterile tourniquet is inflated to 300 mm Hg. The incision is carried down through the skin and lateral fascia but not through the muscle fascial layer. The incision should be an inch longer than the planned bone cuts at both ends. Self retainers are placed at either end of the wound and are repositioned as needed during the case. A lap pad is used to push the peroneal muscles forward into the wound, and a scalpel is used to reflect the muscles off the lateral fibula. The periosteum is not to be broached at this time. A thin layer of muscle, one to two mm in thickness, is left on the fibula, such that there is a slight marbling effect of the muscle on the periosteum. Anteriorly and posteriorly the exposed fascias are incised with a knife. Posteriorly at the distal tip there is a thick fascial layer which is cut on the bone at this time in order to afford exposure of the distal pedicle. Anteriorly, a right angle dissector is run directly on the bone removing all muscle from the fibula. There are no feeding vessels of the fibula on the anterior surface, so there is no danger in this maneuver. After this, deep in the wound the interosseous membrane is visible. The fascial layer is incised with a scalpel. Posteriorly, after the deep fascial layer is incised the flexor hallucis longus is visible. The pedicle is directly under this muscle so care must be taken in its release. Using Metzenbaum scissors the muscle is first spread between its fibers along the entire incision. A finger is hooked around several fibers at a time bringing them forward into the wound. The scissors are used to directly cut the fibers with careful attention to any muscle perforators which are cauterized. If the muscle is stripped, in the same manner as the anterior muscle, then the pedicle will be reflected from the fibula. The muscle is slowly cut in this manner until the pedicle and the interosseous membrane are visible in the depths of the wound. The posterior tibial bundle will also be seen and can be mistaken for the peroneal pedicle. The fibula is cut at this time. A right angle clamp is used to create a tunnel at the two bone cut areas. It is important to stay directly on bone. With the clamp under the fibula and protecting the pedicle two malleable ribbon retractors are placed. A gigli saw is then used to cut the fibula. Care must be taken to hold the fibula in the wound during the second cut or the vascular pedicle will be pulled from the bone. A bone clamp is placed around the freed fibula to use as a handle for dissection. In the distal wound the pedicle is dissected free from the muscle and medium hemoclips are used. There is often a branching of the pedicle proximal to the bone cut, and if both branches are not clipped, during dissection the pedicle can be torn from the fibula. Anteriorly, the extensor hallucis longus has some slips onto the fibula which can be bluntly freed from the bone. Perforators are cauterized with the bipolar. The pedicle should be obvious through the interosseus membrane. The dissection plane is then carried up through the membrane with care paid to the deep perforators. The fibula is swung in the wound during dissection so that no perforators are missed. In a large percentage of cases a large soleal perforator will be seen at the proximal cut. This is too large a vessel for cautery and must be clipped. Often, part of the nerve to the flexor hallucis longus runs with the pedicle. The sacrifice of this nerve cannot always be avoided but does not seem to have any effect on the outcome. The self retainers are removed and the assistant uses two thyroid retractors- one on the anterior fascia and a second pulling posteriorly on the proximal stump of the fibula. Careful blunt dissection can be carried down to the bifurcation of the pedicle. Five centimeters of pedicle is the optimal length that should be obtained before placing two large clips across the pedicle and cutting distally. The fibular graft is then freed from the leg. The tourniquet is then deflated with the retractors in place to examine for bleedi wound is packed with wet lap pads. It is closed later over a drain. The fascial layers are left open. Only the subcutaneous layer and the skin are closed. The leg is then put into a buly dressing. Final preparation of the fibula occurs on the back table. The pedicle is immediately injected with 40 cc of heparinized solution. Both veins and the artery are infused. The pedicle is reflected off the proximal fibula until a large perforating lava vessel is found entering the cortex. If the pedicle length is not at least 5 cm in length the bundle is dissected further back. If the pedicle branches before that occurs, then both branches are preserved with subperiosteal dissection. When the feeder vessel is located, the fibula is cut, at that point, with a reciprocating saw under copious irrigation. The end of the pedicle is then developed with microsurgical dissection. One vein is chosen as the recipient and the other has a small hemoclip placed on the end. The artery and good vein are dissected free for 2 cm from the pedicle proper. They are periodically infused with heparinized solution. The final measurement from the calibrated bone impacter is used to design the second distal bone cut. The periosteum is not rolled back from the end. Absorbable suture is used to bind the pedicle to the distal end of the fibula in order to prevent stripping of the pedicle during insertion into the reamed tunnel in the femoral neck.
____________________________________________
Residual functional deficit after partial fibulectomy for bone graft.
Function following partial fibulectomy.
The effects of resection of the proximal part of the fibula on stability of the knee and on gait.
Biological and physical properties of autogenous vascularized fibular grafts in dogs.
Donor site morbidity following resection of the fibula.
Secondary Reconstruction after Vascularized Fibular Transfer.