
- Discussion:
- restoration of heel width / height requires reduction of tuberosity fragment to sustentacular fragment;
- generally the tuberosity fragment needs to be brought out of varus and a medially displaced position;
- key toreduction of sustentaculum talus fragment, which is almost always in anatomic position in relation to the talus;
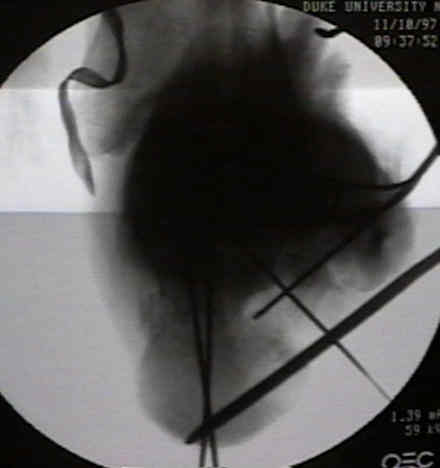
- reduction is facilitated by insertion of a threaded pin into the base of tuberosity fragment;
- pulling the fragment laterally will help bring it out of varus;
- pulling the base of the tuberosity plantarly will help restore Bohler's angle
- the surgeon can pass a finger behind the posterior facet (and over the tuberosity) in order to palpate the superomedial fragment;
- pulling on traction pin and pushing w/ surgeon's finger should effect reduction between tuberosity and sustentaculum;
- tuberostity fragment is opposed to sustentacular fragment and held with K wires directed from the plantar aspect of the heel into the sustentacular fragment;
- a Harris heel view, is required at this time, inorder to confirm the reduction (along the medial wall);
- at this point, heel width should be corrected;
- w/ dislocation of superomedial fragment, there may be entrapment of the FHL, which prevents reduction;

- restoration of heel length:
- a lateral view is taken to assess length and Bohler's angle;
- the tuberosity is pulled out to length, and can be held with K wires driven into the posterior tuberosity which are directed anteriorly to the anterior facet;
- fracture fixation:
- direct a 3.5 mm cortical screw or cannulated screw from the subchondral bone of the posterior facet into sustenacular fragment;
- usually these screws must be directed anteriorly inorder to engage the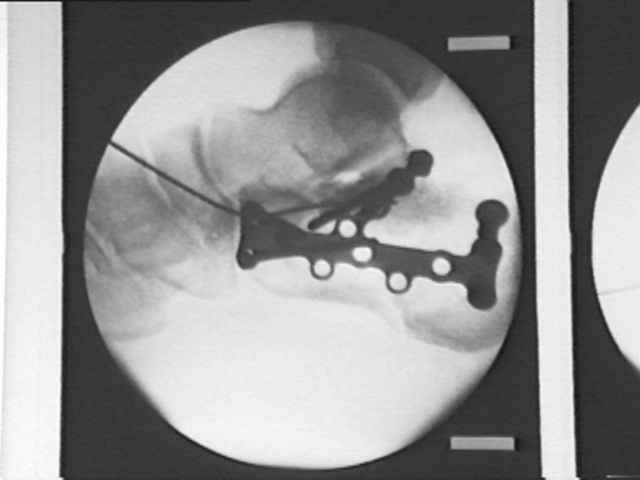 sustentacular fragment;
sustentacular fragment;
- more anterior screw needs to be angled upwards;
- posterior screw is angled downwards into dense area of bone;
- use washers if needed;
- these screws will support the fractured articular segments inaddition to securing the sustentacular fragment;
- alterantively consider use of 4.0 cancellous screws rather than bicortical 3.5 mm cortical screws (even for fixation of the medial fragment);
- as pointed out by Bailey, et al., 4.0 mm cancellous screws provided just as good fixation as 3.5 cortical screws since mechanical failure will occur thru ligament disruption rather than screw pullout;
- Intraarticular calcaneus fractures: a biomechanical comparison or two fixation methods.
- Hazards:- be aware that bicortical fixation of the medial fragment has a high risk of injurying the FHL, nerves, and vessels;
- wires placed in the subchondral bone of posterior facet or anteior to the critical angle of Gissane are at high risk for N/V injuries;
- avoid medial penetration of the posterior facet:
- be aware that the posterior facet slopes from lateral-superior to medial-inferion, and therefore screws which are inserted in a horizontal direction at the superior margin of the posterior facet will penetrate the articular surface;
- in the report by Jordan C, et al (1999), the authors recommend the following:
- at the anterior aspect of the posterior facet, screws need to be angled 5 deg in a plantar direction or need to be placed 1.5 mm below the edge of the articular surface;
- at the mid portion, screws need to be angled 20 deg inferiorly or 10 mm below the joint edge;
- at the posterior portion, screws need to be angled 32 deg inferiorly or 15 mm below the joint edge;
- references:
- Determining the angle of screw placement for internal fixation of calcaneal fractures.
- Internal Fixation of Calcaneus Fractures: An Anatomical Study of Structures at Risk.