
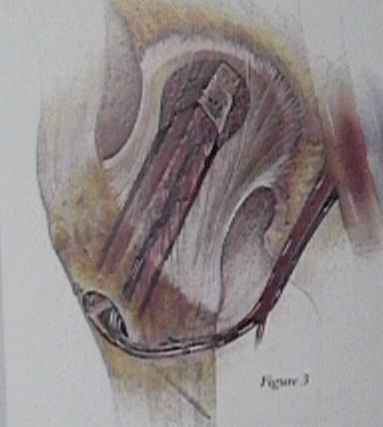
- Technique: The approach to the femur is carried down, through a slightly anteriorly curved 20 cm incision, to split the interval between the fascia lata and the gluteus medius. A large Charnley retractor is used throughout the case for the fascial retraction. The deep plane of dissection is between the rectus femoris and the vastus intermedialis. This plane is held open with two straight self retainers attached to the Charnley retractor with a sponge to ensure no movement occurs. A large self retainer is often needed at the superior wound. The donor vessels originate from the lateral circumflex vessel and course laterally between these two muscles. There are three branches which come forward into the wound: ascending, transverse, and the descending. Unless care is taken in the dissection the desired vessels- ascending branch artery and veins - will be missed. For better visualization, the bridge of aponeurosis between the anterolateral femur and the rectus femoris is taken down. This bridge, known as the falx, is taken down off the anterolateral corner of the femur at the junction of the deep quadriceps muscles. The area beneath the falx is covered with a fat pad, which is swept off to reveal the ascending vessels. At this time if any fat is overhanging the area it is removed with the scissors in order to make the anastamosis easier. The artery and the two veins are visualized. They are mobilized with careful attention to length. Four centimeters of length from the first branch is usually easily obtained. Starting at the anterior part of the wound small hemoclips are placed on any small branches before dividing in order to gain this length. A hemoclip is placed on the end of each of the 3 vessels and they are left deep in the wound for later anastamosis. All the retraction devices are then removed from the wound.
Original Text by Clifford R. Wheeless, III, MD.