
- See: Hallux Valgus:
- Cresentric Proximal Osteotomy:
- allows redirection of the MT without loss of bone neither shortens nor lengthens the first metatarsal;
- complications include malunion, delayed union, non union, and transfer metatarsalgia (not from shortening but if first MT is dorsiflexed);
- Technique of Concentric Osteotomy:
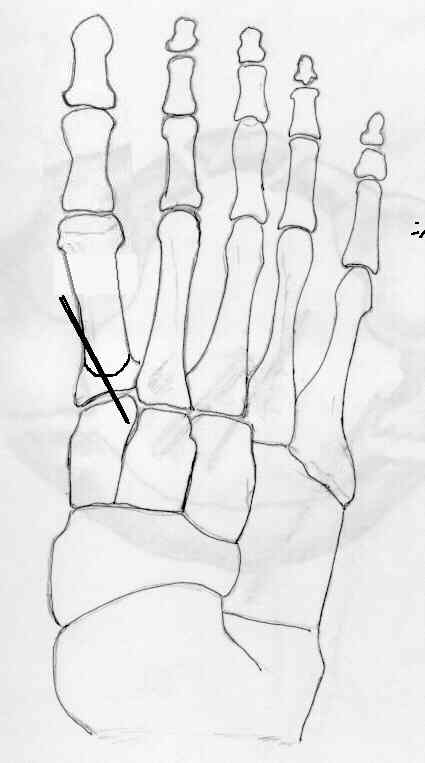
- dorsal incision is made over the base of the first metatarsal, and is carried down just lateral to extensor tendon;
- expose metatarsal-cuneiform joint is identified w/ a needle;
- osteotomy is made approximately 1 to 1.5 cm distal to metatarso-cuneiform joint;
- it can be made either concave proximal or distal;
- ensure that the osteotomy is in a straight dorsal to plantar direction;
- because the 1st metatarsal is angled 30 deg off the floor, the surgeon should tilt the saw 30 deg from the perpendicular of the metatarsal shaft;
- first metatarsal is rotated inorder to correct intermetatarsal angle;
- stabilizing the proximal fragment (small periosteal elevator or osteotome levered under the fragment in the 1-2 interspace) will
facilitate correction of distal fragment (IMA less than 10 deg)
- the distal fragment is rotated laterally about 2-3 mm;
- fixation:
- osteotomy site is fixed w/ single oblique 5/64 Steinmann pin or w/ lag screw;
- if a 5/64 in Steinmann pin is to be utilized, it is driven into the tarsal bones and left extending out of the skin about 5 mm;
- there is some evidence, that a single screw does not provide enough fixation, especially if the patient is noncompliant;
- x-rays are taken to assess correction;
- this having been achieved, begin soft tissue reconstruction;
- Complications:
- type of intrinsically unstable osteotomy if wt bearing distracts osteotomy making stability completely dependent on fixation devices until union occurs;
- transfer metatarsalgia:
- note that medialization of the metatarsal shaft also tends to shift it dorsally;
- this dorsal shift tends to unload the first metatarsal head and transfer the load laterally;
- patients w/ a short first metatarsal or w/ a pronation deformity of the forefoot are at higher risk for this complication;
- it has also been noted that non compliance with wt bearing restrictions may cause a progressive elevation of the metatarsal
following surgery (leading to dorsal malunion);
- this complication may be more common with a proximal concentric osteotomy, especially if there is inadequate fixation
Late results after correction of hallux valgus deformity by basilar phalangeal osteotomy.
Strength of fixation constructs for basilar osteotomies of the first metatarsal.
Osteotomy of the first metatarsal base for metatarsus primus varus.