
- Discussion:
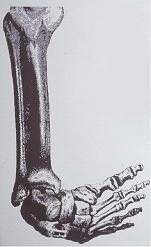
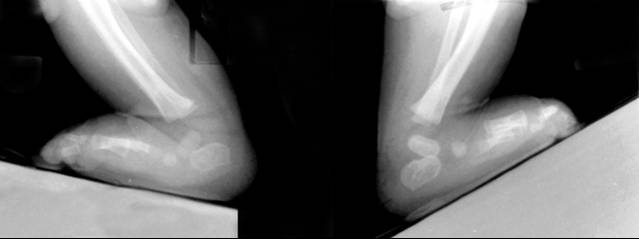
- pathoanatomy:
- whole foot is in extreme supination, however, the fore part of the foot is pronated with respect to the hindfoot, as a result of
the cavus deformity (the first metatarsal is more plantar flexed than the fifth metatarsal);
- navicular and the cuboid are rotated medially in relation to the talus, and are held in adduction and inversion by contracted
ligaments and tendons;
- tibial-navicular interval:
- distance between the medial malleolus and the tuberosity of the navicular;
- shorter intervals indicate worse deformity;
- degree of resistance of navicular to be moved away from medial malleolus correlates with severity of deformity.
- note that in severe clubfoot, complete reduction of the extreme medial displacement of the navicular may not be possible
by manipulation;
- timing:
- casting begins in the first week of life inorder to take advantage of the initial elasticity of contracted ligaments, joint capsules
and tendons;
- improvements from manipulation are maintained by immobilizing the foot in a plaster cast for five to seven days;
- within the first 2-3 months, the surgeon attempts 5-6 manipulation and cast applications;
- children who present for treatment after four or five months old may require operative correction because ligaments become stiffer;
- total duration of treatment should be less than three months;
- 6-8 toe-to-groin plaster casts, changed weekly after manipulation and worn for 7-10 weeks, should be sufficient to obtain
maximum correction possible;
 - Sequence of Correction: (Ponsetti)
- Sequence of Correction: (Ponsetti) - correction of cavus:
- cavus deformity must be corrected prior to correcting the other deformities;
- forefoot is supinated and the first metatarsal is dorsiflexed;
- this reverses the contracted forefoot pronation;
- pronation of the foot will worsen the deformity and will increase the cavus;
- an attempt to correct the inversion of the foot by forcible pronation of anterior part of the
foot increases the cavus deformity as first metatarsal is plantar-flexed further;
- correction of adduction and heel varus:
- goal is to abduct the supinated foot under the talus;
- again, forceful pronation of the foot is avoided since it increases the cavus deformity,
causes mid foot break down and does not address the varus heel deformity;
- talus is rotated laterally so that the foot abducts underneath the talus which is fixed in the ankle mortice;
- this causes lateral rotation of navicular, together w/ cuboid & anterior aspect of calcaneus, w/o pronation of foot;
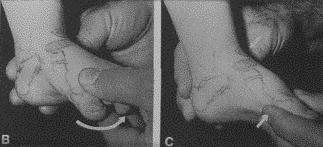
- to correct the varus and adduction, the foot in supination is abducted while counterpressure is applied with
the thumb against the head of the talus;
- foot is abducted in flexion and slight supination to stretch the medial tarsal ligaments, while counter pressure applied on
the lateral aspect of the head of the talus;
- this allows the calcaneus to abduct under the talus which correction of the heel varus;
- heel must not be touched during this manipulation;
- calcaneus abducts by rotating and sliding under the talus;
- noted that the calcaneus can evert only when it is abducted (laterally rotated) under the talus.
- as the calcaneus abducts it simultaneously extends and everts which corrects the heel varus;
- note that the calcaneus cannot evert unless it is abducted;
- casting involves a toe-to-groin plaster cast w/ knee flexed 90 degrees and the foot in maximum external rotation;
- maintenance of correction of varus deformity of hind part of foot which requires external rotation of foot distal to talus;
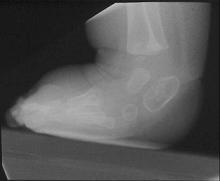
- radiographs may be taken at this point inorder to confirm that the talonavicular joint is reduced, prior to managing equinus;
- cautions:
- avoid forced external rotation of the foot to correct adduction while the calcaneus is in varus;
- this causes a posterior displacement of the lateral malleolus by externally rotating the talus in the ankle mortice.
- avoid abducting the foot against pressure at the calcaneocuboid joint the abduction of the calcaneus is blocked, thereby
interfering with correction of the heel varus
- correction of equinus:
- equinus is corrected last, by dorsiflexion of foot w/ heel in valgus angulation;
- if foot is dorsiflexed prior to correction of the hindfoot varus, rocker bottom foot may be created;
- equinus is corrected by dorsiflexing the fully abducted foot;
- correction entails stretching of the tight posterior capsules and ligaments of ankle and subtalar joints and the tendo achillis;
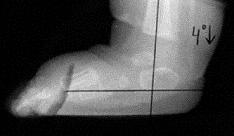
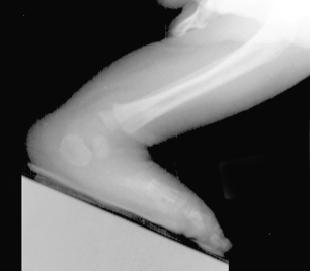
- lateral x-ray are helpful in assessing quality of cast correction;
- percutaneous tenotomy of the achillis tendon:
- may be necessary inorder to avoid rocker bottom deformity;
- dorsiflexion of ankle to > 10 to 15 degrees is rarely possible because of talar and calcaneal malformations
and tight ligaments;
- cautions:
- care should be taken not to cause a rocker-bottom deformity, which can occur when dorsiflexion of foot is attempted w/
pressure under metatarsals rather than under the mid-part of foot, particularly when varus deformity of heel has not
been corrected;
- do not to exert excessive upward force on metatarsals, because this can result in midfoot break (rocker-bottom
deformity);
- ref: Radiographic Evaluation of Idiopathic Clubfeet Undergoing Ponseti Treatment
- Complications:
- increased cavus deformity;
- rocker-bottom deformity;
- longitudinal breach
- flattening of the proximal surface of the talus
- lateral rotation of the ankle
- increased stiffness of the ligaments and joints;
- recurrence:
- Ponsetti advocates use of shoes attached to a bar in external rotation for three months full-time and at night for 2-4 years
Masters in Surgery



Motivation for Ponsetti Method: Current Surgical Methods:


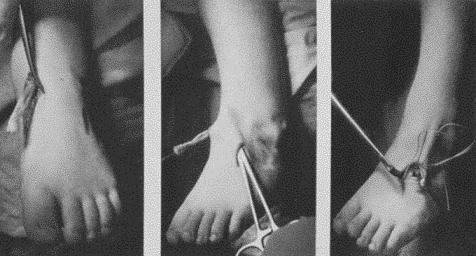
Example of Wound Breakdown following Surgery:


Casting Considerations for the Ponsetti Technique: 1

Casting Considerations for the Ponsetti Technique: 2









Achilles Tenotomy:


Use of x-rays to assist with achilles tentomy:





Dennis Brown Bar:


Outcomes:









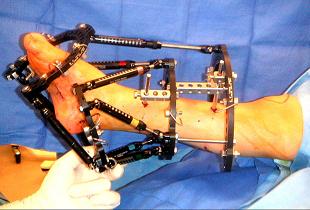
Surgical Case Example: Ilizarov Method




Compliance:

Ponseti Versus Traditional Methods of Casting for Idiopathic Clubfoot
Long term results of treatment of congenital clubfoot.
Congenital club foot: the results of treatment.
Ponseti versus traditional methods of casting for idiopathic clubfoot.
Results of an accelerated Ponseti protocol for clubfoot.
Early Clubfoot Recurrence After Use of the Ponseti Method in a New Zealand Population
Calf Circumference Discrepancies in Patients With Unilateral Clubfoot: Ponseti Versus Surgical Release
Ponseti Method Compared with Surgical Treatment of Clubfoot. A Prospective Comparison