
 - See:
- See: - Radiographic Findings
- Sliding Hip Screw w/ Unstable Frx
- Discussion:
- it is important prior to reduction to distinguish between unstable and stable frx intertroch fractures;
- w/ cortical instability on one side of frx owing to cortical overlap or destruction, frx tends to collapse in direction of instability;
- truly stable intertrochanteric frx, therefore, is one that, when reduced, has cortical contact w/o a gap medially & posteriorly;
- this contact prevents frx displacement into varus or retroversion;
- in some cases, an unstable frx pattern may be missed due to an inadequate lateral radiograph, which interferes w/ assessment of size postero-medial comminution and presence of coronal split in the greater trochanteric 4 part frx; 
- the dreaded complication of unstable intertrochanteric fractures is migration of the femoral head into varus and retroversion;
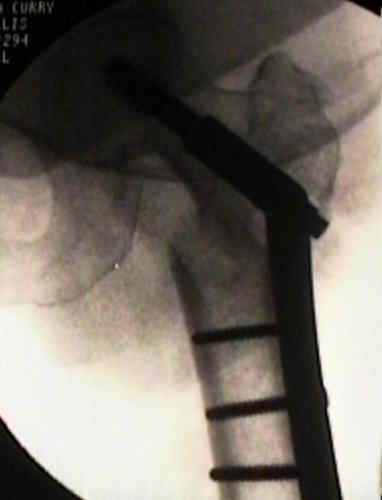
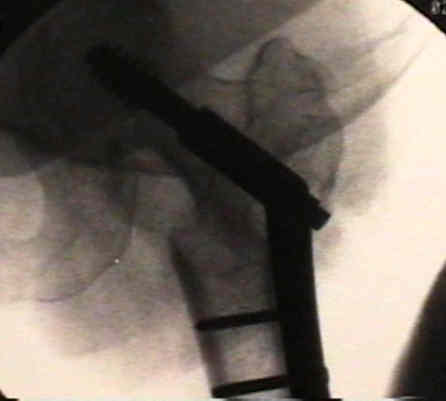
- internal fixation of frx in varus position:
- frx stability exists exits in the displaced position because of medial contact between the two major fragments;
- this type of fixation is the least satisfactory type of nonanatomical reduction because of the limp and shortening that result from union in the displaced varus position; 
- hazards:
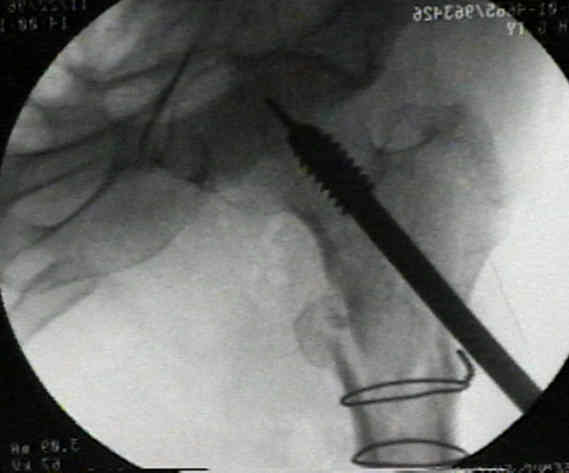
- avoid treating unstable fractures like stable ones (ie. avoid the following);
- in this case, there was unacceptable frx opposition;
- frx shortening of 6-7 mm does not affect ambulation but shortening of 13-18 mm of shortening will affect ambulation;
- frx shortening or collapse will affect the abductor lever arm and will lead to abductor weakness;
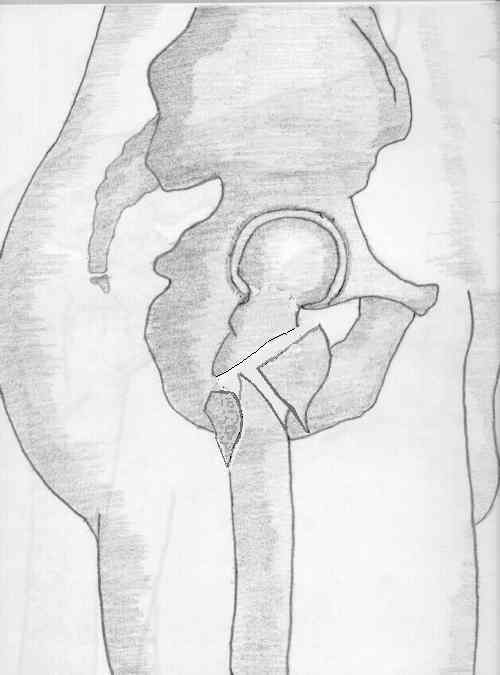
- Types of Unstable Frx
- lesser trochanter frx
- stability is lost when the less troch contains a portion of the calcar;
- greater trochanter:
- comminution of greater trochanter & adjacent posterolateral shaft predispose to medial shaft migration;
- there is no contact between proximal & distal frag owing to comminution and displacement of frx frag medially and posteriorly;
- type IV frx (see classification)
- when using a 150 deg plate, the head and neck segments often must be placed in valgus inorder for the guide wire to reach the center of the femoral head;
- this valgus positioning tends to open up the postero-medial gap, in which case a modified Sarmiento osteotomy is needed inorder to re-establish frx opposition;
- using a 135 deg plate, a lesser amount of valgus positioning was required and therefore a smaller posteromedial gap was created;
- 4 part frx:
- as noted by Den Hartog BD, et al. (1991), mean load to failure was increased in unstable intertrochanteric fractures by re-establishment of medial contact (using an osteotomy, use of a high angle plate, and placement of the lag screw in center of the femoral head;
- w/ a severely comminuted 4 part frx (in which case, it is not possible to convert the unstable frx to a stable one), one can consider a type of modified Dimon and Hughston's Osteotomy;
- reversed obliquity:
- tendency toward medial displacement of shaft 2nd to hip adductors;
- ref: Treatment of the unstable intertrochanteric fracture. Effect of the placement of the screw, its angle of insertion, and osteotomy

- IM Hip Screw
- Treatment of Unstable Frx with Sliding Hip Screw and Plate:
- compared to a medial displacement osteotomy, an anatomic reduction is more able to load the medial cortex in patients w/ an unstable intertrochanteric fracture;
- often there will be posterior displacement of the distal fragment, which requires a strong assistant to lift the fragment upwards with a bone hook;
- references:
Biomechanical evaluation of anatomic reduction verus medial displacement osteotomy in unstable intertrochanteric fractures.
- stability may be restored by osteotomy or medial displacement;
- Sarmento's osteotomy
- Dimon and Hughston's technique
- Wayne County Reduction
- strength of the fragment implant assembly is determined by:
- bone quality
- fragment geometry
- reduction
- implant placement
- implant design
- trochanteric stabilization plate is designed to fit onto the 135 deg DHS plate and helps prevent excessive lateral sliding of the proximal frx fragments (and excessive shortening);
- frx shortening of 6-7 mm does not affect ambulation but shortening of 13-18 mm of shortening will affect ambulation;
- frx shortening or collapse will affect the abductor lever arm and will lead to abductor weakness;
- references:
- Dynamic hip screw with trochanteric stabilizing plate in the treatment of unstable proximal femoral fractures: A comparitive study with Gamma Nail and Compression hip screw.
- Clinical results using the trochanter stabilizing plate (TSP): The modular extension of the dynamic hip screw (DHS) for internal fixation of selected unstable intertrochanteric fractures.
case examples:








Axial loading studies of unstable intertrochanteric fractures of the femur.
Unstable intertrochanteric/subtrochanteric fractures of the femur.
Medial displacement osteotomy for unstable intertrochanteric fractures. Twenty years later.
How effective are osteotomies for unstable intertrochanteric fractures?