
(see also: Technique of Reduction)
Discussion
initial considerations
- angular / rotational deformity: (growth will not correct rotational deformity)
- age
- distance from physis
- direction of angulation
- amount of deformity
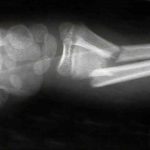
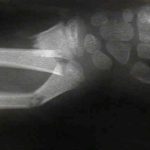
bayonette apposition
- generally bayonette opposition will require operative reduction (either closed with a Kapandji K wire levering technique or in some situations, an open reduction and fixation with K wires will be required);
- historically, overriding of a both bones forearm fracture was acceptable if...
- there was no deviation of radius and ulna toward each other;
- there was no encroachment of the interosseous space;
- pt is less than 10 yrs of age;
in pts < 6 yrs of age
- up to 15 deg of angulation is acceptable, especially if frx is distal;
- 5 deg of rotation may also be acceptable;
between ages of 6-10 yrs
- less than 10 deg of angulation should remodel especially if frx is close to distal epiphysis;
- bayonet apposition may be acceptable, although end to end apposition is preferred;
- acceptable angulation is less than 15 deg, however, even more angulation may be preferable to resorting to open reduction;
- this is especially true if the reduction allows physiologic pronation and supination;
pts > 12 yrs of age
- no angulatory or rotational deformity is considered acceptable;
- more aggressive treatment is required, including open reduction and compression plating may be required;
Displaced Distal Third Frx
- angulation up to 20-25 deg during first ten years is OK;
- angulation > 10 deg is unlikely to correct after 10 yrs

References
- The effects of angular and rotational deformities of both bones of the forearm. An in vitro study.
- Remodelling potential of the growth plate following angular osteotomy of the long bones in baboons. Abraham E, Groya RJ: Trans Orthop Res Soc 1981;6:266.
- Angular remodeling of midshaft forearm fractures in children.
- Spontaneous correction of deformity following fractures of the forearm in children.
- Accurate prediction of outcome after pediatric forearm fracture.
- Bowing fractures of the forearm in children: a long-term followup.
- Closed Treatment of Overriding Distal Radial Fractures without Reduction in Children