
- See: Fracture Dislocation / Anterior Instability
- Discussion:
- posterior dislocation is rare & should raise possibility of seizure as cause, other causes include an electric shock or ECT without
muscle relaxants;
- mechanism:
- axial loading of the adducted, internally rotated arm;
- because the internal rotator muscles are approx twice as powerful as the exernal rotator muscles, a sudden contraction (such
as from a seizure or shock) will cause the humeral head to dislocate;
- involuntary recurrent posterior subluxation may be associated w/ high forces generated during follow thru phase of
various sports activities;
- this develops as humerus is in adduction, flexion, and internal rotation, & maximal contractions of subscapularis and deltoid;
- see throwing injuries of shoulder
- ref: The aetiology of posterior glenohumeral dislocations and occurrence of associated injuries
- voluntary dislocation:
- Electromyography in voluntary posterior instability of the shoulder
- risk factors:
- reverse Bankhart (detachment of posterior labrum);
- defect of the anterior portion of the humeral head (reverse Hill Sachs)
- increased retroversion of the humeral head or retroversion of the glenoid;
- posterior glenoid deficiency;
- ref: Posterior Shoulder Instability: Does Glenoid Retroversion Predict Recurrence and Contralateral Instability?
- note that posterior dislocation is distinguished from recurrent posterior instability (this is associated with generalized laxity and is
only associatted with a documented posterior dislocation in about 23% of cases);
- posterior instability is often associated with multidirectional instability;
- Physical Exam:
- 3 types of the posterior instability may be found:
- unidirectional
- bidirectional (inferior and posterior instability)
- multidirectional (anterior, inferior, and posterior):
- references:
- Recurrent posterior instability (subluxation) of the shoulder.
- Recurrent posterior shoulder instability. Diagnosis and treatment.
- posterior apprehension test:
- posterior translation stress is applied to the arm which is placed in flexion, adduction, and internal rotation;
- w/ frank dislocation, pt usually presents with arm adducted and internally rotated, and attempts at abduction and external
rotation are painful;
- inability to externally rotate in neutral position;
- inability to supinate;
- the coracoid process appears prominent;
- w/ chronic undreduced dislocation, exam may resemble frozen shoulder;
- Radiographs: 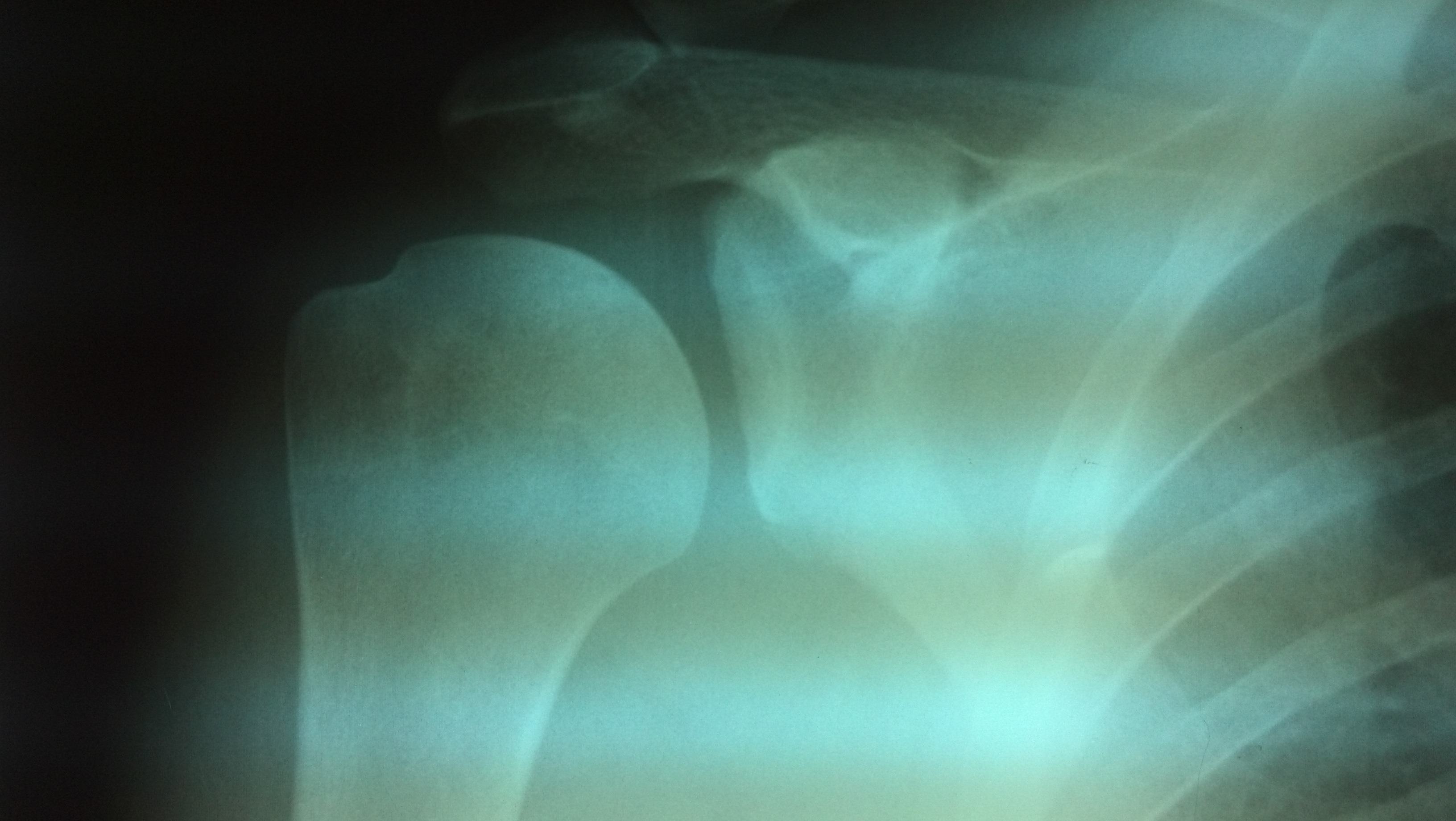
- Reverse Hill Sach Lesion
- compression fracture of the anteromedial portion of the humeral head is produced by the
posterior cortical rim of the glenoid;
- references:
- Excessive retroversion of the glenoid cavity. A cause of non-traumatic posterior instability of the shoulder
- Non Operative Treatment:
- indicated for defects less than 20%;
- involves strengthening of the external rotators (infraspinatus);
- Operative Treatment: Arthroscopic Options: (see anterior reconstruction)
- posterior capsule imbrication: (see arthroscopic knots)
- rotator interval lesion
- accessory posterior portal:
- created 2 cm inferior to the posterolateral acromial angle;
- this is about 1 cm lateral to a standard posterior glenohumeral portal
- improves access to the posteroinferior aspect of the glenoid labrum and capsule;
- posterior band of the inferior glenohumeral ligament is identified;
- goal is to shift the posterior capsule approximately 1 cm superior, opposing the shifted the capsule to the labrum
(assumming no labral tear);
- superiormost suture was placed at the level of the biceps insertion (see slap repair)
- labral pathology:
- incomplete stripping / separation without displacement
- marginal crack / incomplete avulsion
- chondrolabral erosion / loss of contour
- flap tear
- references:
- Management of the failed posterior/multidirectional instability patient
- Posterior instability of the shoulder following thermal capsulorrhaphy for multidirectional instability.
- Arthroscopic posteroinferior capsular plication and rotator interval closure after Bankart repair in patients with traumatic anterior glenohumeral instability�A minimum follow-up of 5 years.
- A biomechanical analysis of shoulder stabilization: posteroinferior glenohumeral capsular plication.
- Posterior shoulder instability secondary to reverse humeral avulsion of the glenohumeral ligament.
- Arthroscopic management of posterior instability: evolution of technique and results
- Four-quadrant approach to capsulolabral repair: an arthroscopic road map to the glenoid
- Arthroscopic Technique for the Evaluation and Treatment of Posterior Shoulder Instability
- Arthroscopic Posterior Labral Repair and Capsular Shift for Traumatic Unidirectional Recurrent Posterior Subluxation of the Shoulder
- Open Surgical Treatment Options:
- Postero-Inferior Capsular Shift: (Bigliani, et al (1995) and Fuchs B, et al)
- posteroinferior aspect of capsule is shifted superiorly;
- lateral position;
- posterior approach to the shoulder:
- oblique incision across the scapular spine starting at posterolateral apsect of the acromion;
- oblique incise gives nicer scar than verticle scars;
- deltoid is split no more than 5 cm below acromion (deltoid may be split from the scapular spine to enhance exposure);
- careful with axillary nerve:
- The posterior branch of the axillary nerve: an anatomic study
- controversies: deep dissection:
- infraspinatus split approach:
- references:
- Posterior capsulorrhaphy through infraspinatus split for posterior instability. Dreese J, Tech Shoulder Elbow
Surg 2005;6:199-207.
- Infraspinatus muscle-splitting incision in posterior shoulder surgery: An anatomic and EMG study.
- identify the interval between the infraspinatus and the teres minor (infraspinatus is cut and tagged for later closure);
- capsule
- identify the underlying capsule and clear it from the overlying musculature;
- Bigliani et al: capsule is incised 1 cm medial to labral edge (carefult not to injure axillary nerve);
- Fuchs, et al:
- posterior aspect of the capsule is then incised horizontally at the midglenoid level, from the site of the glenoid
attachment to the site of the humeral attachment.
- capsule is then incised vertically about 5 mm medial to its attachment on the humerus (avoid axillary nerve injury);
- T-shaped incision yielded a superior flap and an inferior flap.
- shoulder is dislocated posteriorly and sequential examination of the joint is carried out from anterior to posterior;
- labrum is examined and is repaired if torn;
- capsule is shifted vertically and imbricated;
- superior flap is shifted inferiorly and fixed to the lateral rim of the capsule
- inferior flap is shifted superiorly and fixed superiorly to the lateral capsule;
- outcomes:
- in the study by Fuchs B, et al., the authors reviewed 26 consecutive shoulders which had recurrent, voluntary posterior
subluxation of the shoulder;
- subjective results were excellent for sixteen shoulders, good for eight, and fair for two;
- instability recurred in six (23?%) of the 26 shoulders;
- capsular shift references:
- Shift of the posteroinferior aspect of the capsule for recurrent posterior glenohumeral instability.
- Capsulorrhaphy with a staple for recurrent posterior subluxation of the shoulder.
- Shift of Posteroinferior Aspect of Capsule for Recurrent Posterior Glenohumeral Instability.
- Post-Inferior Capsular Shift for Treatment of Recurrent, Voluntary Posterior Subluxation of Shoulder.
- McLaughlin Procedure:
- involves transfer of lesser tuberosity w/ its attached subscapularis tendon into the defect;
- indicated for defects more than 20% but less than 40% of the joint surface;
- disadvantages: can limit internal rotation of shoulder;
- Arthroscopic Fixation of Subscapularis in Reverse Hill-Sachs for Traumatic Unidirectional Posterior Dislocation of Shoulder.
- Allograft Reconstruction: (see allograft menu)
- involves insertion and fixation of a shaped piece of allograft into the defect;
- indicated for patients w/ greater than 40% defect in the humeral head who have recurrent posterior instability;
- advantages: prevents posterior dislocation w/o limiting internal rotation;
- technique:
- use anterior approach to the shoulder;
- cryopreserved femoral head allograft is shaped to fit into humeral head defect so that outer spherical femoral surface is
congruent w/ humeral surface;
- grafts are fixed to the humeral head w/ a 3.5 mm cancellous lag screws;
- references:
- Recurrent posterior dislocation of the shoulder: treatment using a bone block.
- Treatment of locked chronic posterior dislocation of the shoulder by reconstruction of the defect in the humeral head with an allograft.
- Allograft Reconstruction of Segmental Defects of Humeral Head for Chronic Locked Posterior Dislocation of Shoulder.
- Complications of Posterior Dislocation:
- fractures of the posterior glenoid rim (occurs anteriorly directed forces that push humeral head out posteriorly);
- frx of proximal humerus (upper shaft, tuberosities, and head);
- recurrent posterior instability
The treatment of posterior subluxation in athletes.
Posterior subluxation of the glenohumeral joint.
Locked posterior dislocation of the shoulder: Treatment using rotational osteotomy of the humerus.
Chronic unreduced dislocations of the shoulder.
Rotational osteotomy of the humerus for posterior instability of the shoulder.
Locked posterior dislocation of the shoulder.
Arthroscopic Repair of Circumferential Lesions of the Glenoid Labrum. Surgical Technique