
- Discussion:
- frx consist of frxs of both pubic rami plus posterior frx of SI complex or sacrum:
- there is vertically oriented frx thru anterior and posterior pelvis together w/ superior displacement of lateral "acetabulum-containing" fragment of pelvis;
- this injury is characterized by rupture of entire pelvic floor, including posterior SI complex as well as sacrospinous and sacrotuberous ligaments;
- vertial stability:
- sacrotuberous ligament: stout ligament which exteds to the posterolateral sacrum and dorsal aspect of the posterior iliac spine to the ischial tuberosity;
- posterior sacroiliac ligaments, provides vertical stability to the pelvis.
- injury may be unilateral or bilateral;
- these frx are unstable owing to the significant posterior pelvic disruption;
- usually results from fall from height onto lower limbs;
- Physical Exam:
- displacement in vertical plane is diagnosed by applying one hand to pelvic iliac crest and using other to apply traction to leg which should cause displacement in vertical plane;
- Radiographic Evaluation:
- anterior lesion: (see: anterior pelvic injuries)
- disruption of the symphysis
- disruption of the inferior and superior pubic rami
- disruption of all four rami
- disruption of two rami plus symphysis pubis;
- posterior lesion: (posterior pelvic injury:)
- posterior lesion may be a fracture of ileum
- dislocation or frx dislocation of SI joint
- more than 5-15 mm of cephalic displacement of posterior SI complex on outlet views gap implies instability;
- frx of 4th or 5th lumbar transverse process;
- ref: Fracture of the transverse process of the fifth lumbar vertebra.
- detachment of bony insertion of sacrospinous ligaments from either sacrum or ischial spine are evidence of vertical instability;
- frx of sacrum;
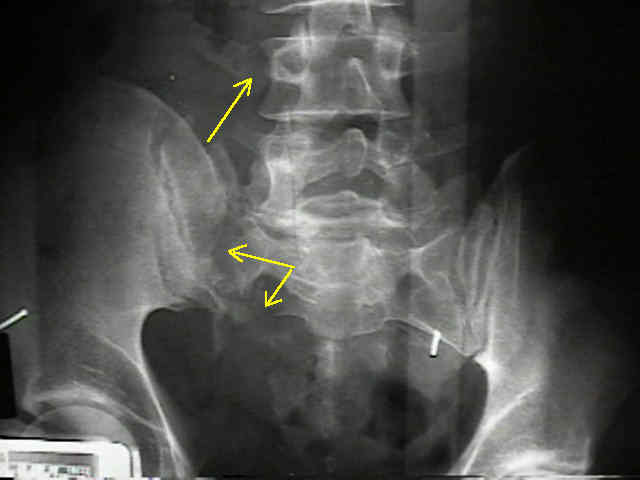
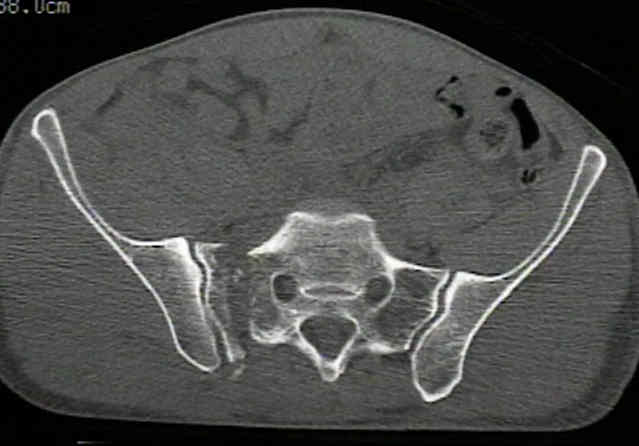
- the following is an example of a Malgaine frx equilavent, in a patient who fell out of a tree;
- the frx appears to have a shear component w/ vertical displacement of the fracture;
- ref:
- The role of standard roentgenograms in the evaluation of instability of pelvic ring disruption.
- Fracture of the transverse process of the fifth lumbar vertebra.
- Is a fracture of the transverse process of L5 a predictor of pelvic fracture instability?
- Initial Management:
- Malgaigne frxs are associated w/ heavy bleeding (see: bleeding from pelvic frx), requiring on average 7-8 units of pRBC;
- if pelvis is unstable w/ vertical migration or posterior displacement, then place of supracondylar femoral pin w/ 25-30 lbs of traction is used to pull the pelvis back down into a reduced position (w/ equal leg lengths);
- approximately one half of patients treated non operatively w/ traction may expect long term low back pain and/or leg discomfort;
- approximately one third will have a pelvic obliquity and/or limp;
- ref: Traction vertical shear pelvic ring fracture: a marker for severe arterial injury? A case report.
- External Fixation:
- serves only as adjunct to other forms of treatment for these frx;
- has little potential to control pelvic frx w/ involvement of SI joint, including sacral frxs & some posterior iliac wing fractures;
- indications:
- isolated pelvic frxs when pt does not require mobilization
- use traction to reduce vertical and/or posterior displacement, while external fixation frame is used to control rotation;
- complex frxs: where internal fixation may not be suitable;
- in the study by Lindahl J, et al (1999), the external fixator failed to give and maintain a proper reduction in 38 of the 40 type-C injuries.
- in type-C injuries more than 10 mm of residual vertical displacement of the injury to the posterior pelvic ring was significantly related to poor outcome;
- in 14 patients in this unsatisfactory group poor functional results were also affected by associated nerve injuries;
- special considerations:
- resistance to verticle displacement is almost doubled by using 5mm rather than 4 mm half pins for iliac wing fixation;
- stability is also enhanced by adding second pin group in each ilium between antero-inferior & superior iliac spines;
- most rigid construction:
- involves combination of SI jont fixation & external frame placed anteriorly;
- ref:
- Failure of reduction with an external fixator in the management of injuries of the pelvic ring. Long-term evaluation of 110 patients.
- Anatomic and radiographic considerations in the placement of anterior pelvic external fixator pins.
- Biomechanical testing of new and old fixation devices for vertical shear fractures of the pelvis.
- External fixation of unstable Malgaigne fractures: the comparative mechanical performance of a new configuration.
- Unstable fractures of the pelvis treated by external fixation.
- The Role of External Fixation in Pelvic Disruptions.
- Posterior Fixation:
- SI jont fixation
- Vertically unstable pelvic fractures fixed with percutaneous iliosacral screws: does posterior injury pattern predict fixation failure?
- sacral bars:
- safest method of stabilizing a sacral fracture is to use sacral bars;
- these bars pass from one posterior superior spine to other, thereby making direct fixation of fracture w/ lag screws unnecessary;
- two sacral bars are used to prevent rotation;
- bars must be posterior to sacrum to avoid entering sacral spinal canal
The pathological anatomy of Malgaigne fracture-dislocations of the pelvis.
Critical analysis of results of 53 Malgaigne fractures of the pelvis.
Femoral Shaft Fractures Associated With Unstable Pelvic Fractures.
Open reduction and internal fixation of vertical shear pelvic fractures
Original Text by Clifford R. Wheeless, III, MD.
Last updated by on Thursday, September 6, 2012 1:42 pm