

Case Example by Dr. James R. Urbaniak MD
- Discussion:
- indicated for patients with basal joint arthritis or CMC instability;
- LRTI involves partial or complete resection of the trapezium and recreation of the palmar oblique ligament using the distally based radial half of FCR
to reconstruct ligamentous support for the metacarpal;
- supporting ligamentous sling is made by passing tendon thru center of base of metacarpal and its unlnar cortex;
- this maintains length and prevents radial subluxation;
- remainding tendon is folded & placed into area of absent trapezium;
- patients can expect significant long term increases in grip and pinch strength following this procedure;
- associated conditions:
- carpal tunnel syndrome occassionally occurs along w/ basal joint arthritis;
- performing a carpal tunnel release along w/ the LRTI incision may spark a flare reaction, or even RSD;
- instead, the decompression can be performed thru the LRTI incision;
- removing the trapezium partially decompresses the carpal tunnel and releasing the remainder of the flexor retinaculum off the
scaphoid, completes the decompression;

- PreOp Planning:
- must determine status of MP, CMC, and STT joint;
- correction of CMC DJD will not eliminate pt's pain if pt has involvement of the STT joint;
- preop x-rays may fail to demonstrate STT degenerative changes;
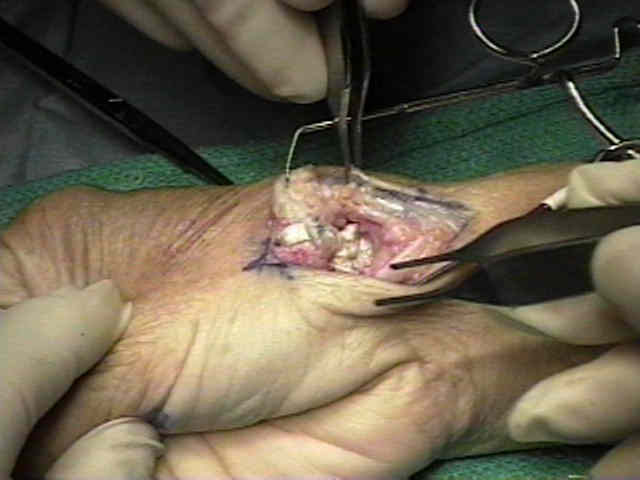
- Surgical Technique:
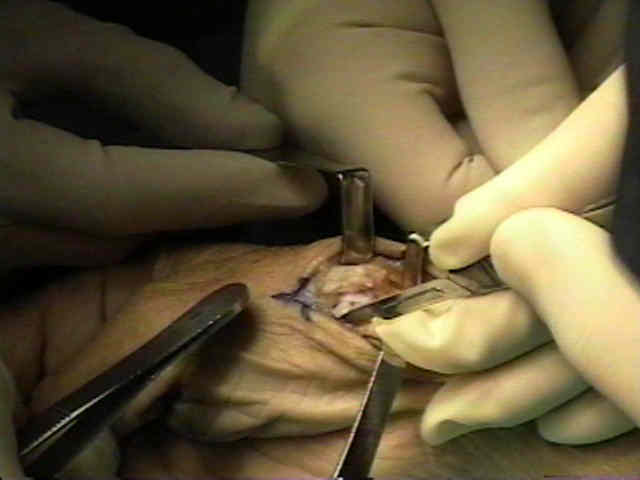
- incision and initial dissection:
- curvilinear incision is made over the volar radial aspect of the CMC joint of the thumb extending volarly at its proximal aspect (volar aspect of snuff box);
- incision should allow access of the FCR and 1st extensor compartment;
- dissection is carried down to the subcutaneous tissue;
- branches of dorsal radial sensory nerve are identified and protected w/ Penrose drain loops;
- thenar musculature is elevated over the volar radial side of trapezium, base of metacarpal, and FCR;




- abductor pollicis longus and EPB are identified and incision is made either between them or along the volar aspect of these tendons;
- radial artery is identified and is retracted dorsally;
- capsule overlying the transtrapezial joint was identified and incised longitudinally on volar-radial side;
- traction on the thumb improves visualization around the trapezium;



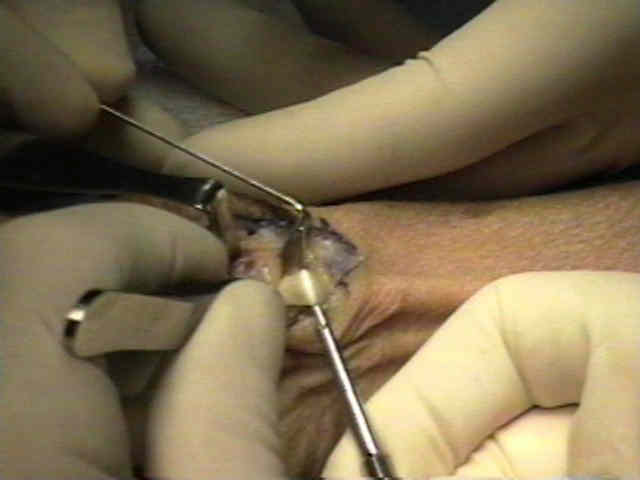
- resection / debridement of the trapezium:
- incomplete trapezium excision:
- this form of treatment is advocated for trapezial DJD on both the CMC side as well as the STT side;
- cited advantages are technical ease and good reported clinical results;
- in the absence of STT arthritis or web space contracture, consider resection of only the distal aspect of the trapezium;
- partial excision is especially considered in younger patients;
- distal trapezial debridement removes both trapezial horns;
- usually the proximal trapezium requires minimal debridement, since there is usually enough space to accomodate interposition of FCR tendon;
- in some cases, the distal scaphoid may require debridement, inorder to allow better adherence of the FCR tendon graft;
- layered FCR tendon is inserted in the STT gap and the CMC gap, or alternatively a drill hole is made through the dorsum of the
trapezium towards the distal trapezium;
- references:
- Ligament reconstruction for the painful thumb carpometacarpal joint: a long term assessment.
- Save the trapezium: double interposition arthroplasty for the treatment of stage IV disease of the basal joint.
- The Scaphotrapezial Joint After Partial Trapeziectomy for Trapeziometacarpal Joint Arthritis: Long-term Follow-up
- complete trapezium excision:
- complete resection of the trapezium is considered if there is preoperative STT arthritis or first web space contracture;
- potential complications of complete resection include shortening and subluxation;
- complete resection of the trapezium will facilitate exposure of the FCR tendon and decreases possible impingement between
thumb metacarpal and trapezium;
- removing the trapezium piece-meal with a rounger is safer than trying to completely excise it with a knife (which risks injury to the FCR);
- during resection of the trapezium, take care to protect the FCR tendon;
- in most cases, the FCR will send a slip to the trapezium;
- having an assistant distract on the thumb will facilitate the excision;




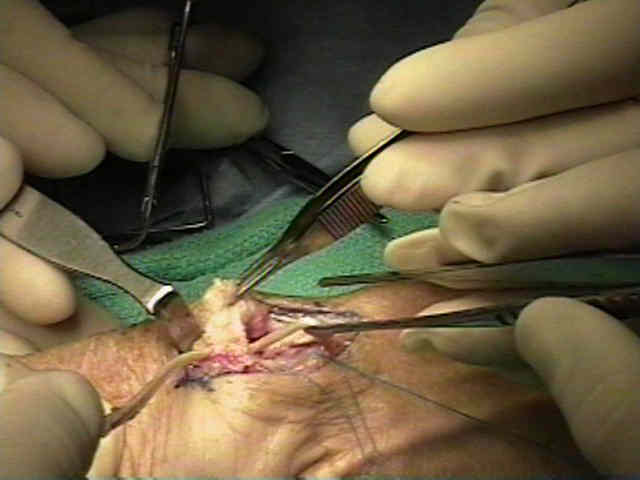
- resection of the metacarpal base:
- metacarpal base is resected w/ care to preserve abductor pollicis longus;
- this increases exposure of the trapezium and allow entry into the medullary canal;

- drilling of metacarpal base:
- a 2.5 mm drill is used to create a hole at the dorsal base of the thumb;
- drill hole is made 1 cm proximal on the dorsal radial aspect in line with thumb nail and exiting the middle of the articular surface
- hole is sequentially enlarged to 6 mm w/ a currette;
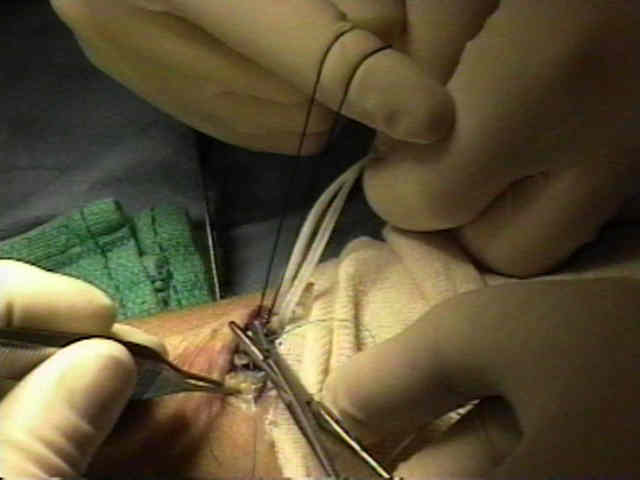
- harvest of the FCR: 
- generally, the distally based FCR tendon graft needs to be 12 cm in length;
- entire FCR tendon harvest:
- in the report by Tomaino, et al 2000, the authors noted that there was no negative impact on wrist function with harvest of the entire FCR tendon for LRTI procedure;
- specifically there were no decline in wrist motion or wrist flexion strength;
- references:
- Use of the entire width of the flexor carpi radialis tendon for the ligament reconstruction tendon interposition arthroplasty does not impair wrist function.
- Trapeziometacarpal arthroplasty using the entire flexor carpi radialis tendon.
- partial FCR tendon harvest:
- through the proximal aspect of the wound, protect the radial artery, and then identify the FCR tendon;
- make a small split in the distal tendon and pass a No 1 nylon suture thru this split;
- make a small transverse incision over the FCR tendon 12 cm proximal to the wrist joint;
- placing tension on the distal FCR tendon will facilitate placement of the proximal transverse incision (usually the incision is made too far radially);
- insert a curved tendon passer over the proximal FCR tendon sheath distally so that exits adjacent to the distal FCR tendon (at the distal wound),
and pull both ends of the nylon suture out of the proximal transverse wound;
- grasp both ends of the suture and use a "back and forth sawing motion" to longitudinally split half of the FCR tendon;
- once the looped end of the suture is delivered into the proximal wound, the tendon is cut at its proximal aspect and retracted through the wound;
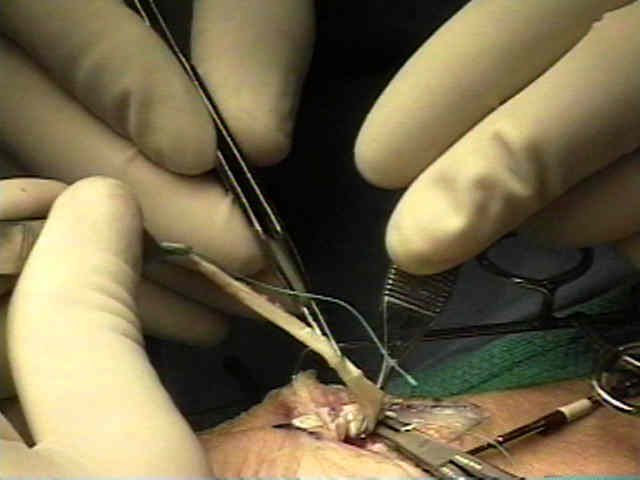
- pass the FCR tendon distally (into the distal wound);
- use a dissecting clamp to tunnel underneath of the radial artery and EPB, inorder to deliver the tendon into the tapezial bed;
- two 4-0 ethibond sutures are placed into the base of the FCR tendon insertion;





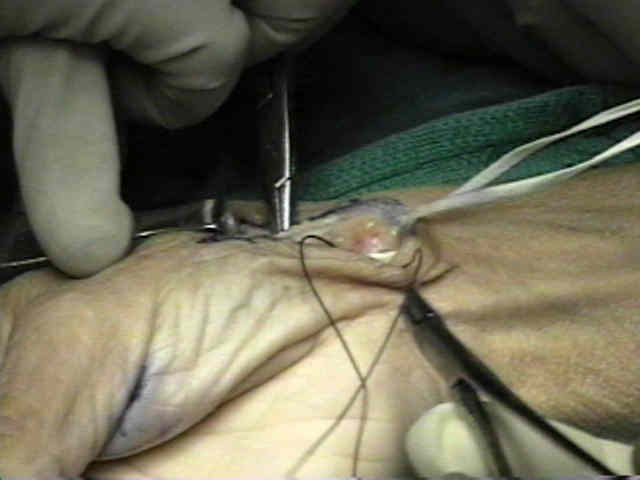

- passage of the FCR:
- FCR tendon is then passed thru the medullary canal and out the metacarpal drill hole;
- the free end of the tendon is passed around this construct inorder to make half of a square knot;
- suture this in place w/ interrupted 4-0 Vicryl suture;




- 0.45 K-wire was then placed across the thumb metacarpal into the index metacarpal after it had been reduced in anatomical position;
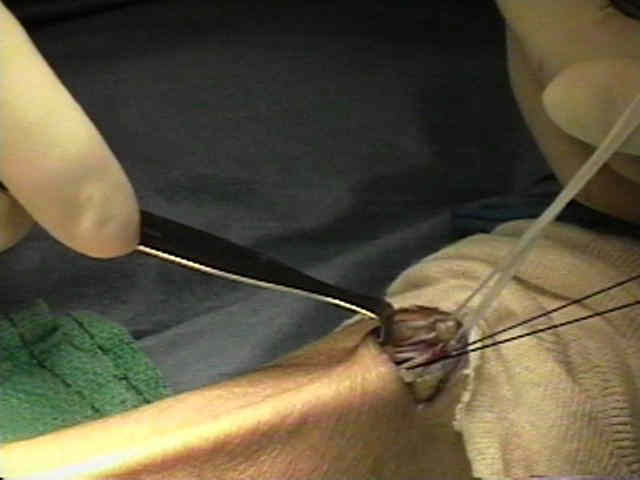
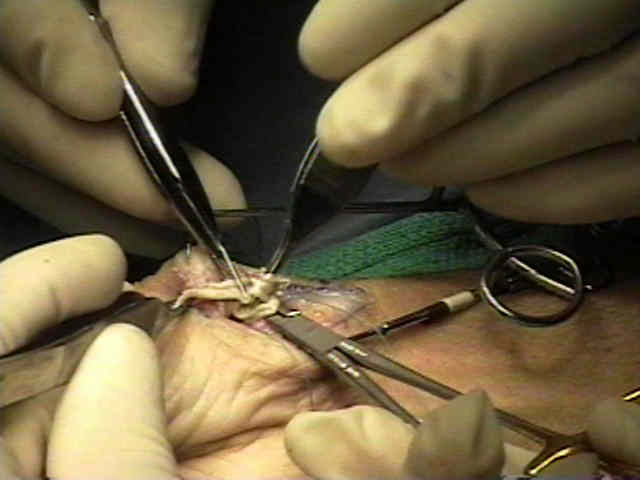
- slightly straighten out the needle of the suture which has been passsed thru the base of the FCR tendon;
- the FCR tendon is then passed back and forwth over the needle in accordian fashion;
- accordian tendon was sutured together using interrupted 4-0 Vicryl suture;
- an additional deep suture is tied over the top of the accordion tendon to hold it snugly in the defect;
- MP joint:
- if there is MP joint hyperextension (more than 20 deg), consider incising the EPB tendon insertion, and inserting it into the distal
thumb metacarpal once the capsule has been closed;
- w/ more than 30 deg of passive MP hyper-extension then stabilization will be required;
- w/o stabilization, ligament attrition may occur;
- surgical options for stabilization include K wire fixation in 10 deg of flexion, volar capsulodesis, or MP fusion;
- references:
- A simplified technique to correct hyperextension deformity of the metacarpophalangeal joint of the thumb.
- Influence of metacarpophalangeal joint position on basal joint-loading in the thumb.
- The role and implementation of metacarpophalangeal joint fusion and capsulodesis: Indications and treatment alternatives.
- wound closure:
- dorsal and ulnar aspect of the capsule are repaired;
- care must be taken not to incorporate the radial artery in capsular closure;
- skin was closed with h 5-0 interrupted and running nylon suture over a TLS drain;
- thumb should be placed in a thumb spica cast for 4 weeks
Arthroplasty of the basal joint of the thumb. Long-term follow-up after ligament reconstruction with tendon interposition.
Carpometacarpal arthritis of the thumb.
Tendon suspension sling arthroplasty for thumb trapeziometacarpal arthritis.
Ligament reconstruction with trapezium retention arthroplasty for carpometacarpal arthritis.